
































































































Medical drug and alcohol detox is the first step in recovery, using round-the-clock medical support to safely manage withdrawal and clear substances from your system.
In this guide, you will learn detox timelines, what to expect during each phase, costs, insurance coverage, and how to choose the right level of care. We also explain why professional detoxification is safer than quitting cold turkey at home, and what happens after detox is complete.
Key Points
- Medical detox safely manages withdrawal under physician supervision, using medications to reduce symptoms and prevent complications.
- Alcohol, benzodiazepine, and opioid withdrawal can be dangerous or life-threatening, so medical supervision is strongly recommended for these substances.
- Detox follows three phases: evaluation, stabilization, and transition into ongoing addiction treatment.
- Most acute detox programs last 3 to 10 days, though protracted withdrawal symptoms can continue for weeks or months.
- Inpatient detox costs roughly $600 to $1,000 per day on average, while outpatient detox costs less but is only safe for milder cases.
- The Affordable Care Act requires most health plans to cover substance use disorder treatment, including medical detox.
In This Article
- What is medical detox?
- Who needs medical detox?
- The three phases of medical detox
- Withdrawal timelines by substance
- Medications used in medical detox
- Inpatient vs. outpatient detox
- How much does medical detox cost?
- Does insurance cover detox?
- Why at-home detox can be dangerous
- What happens after detox?
- How to choose a detox center
- Frequently asked questions
What Is Medical Detox?
Medical detox is a clinically supervised process for safely clearing drugs or alcohol from the body and managing withdrawal symptoms with the support of doctors, nurses, and behavioral health staff. It is the first stage of treatment for many people with a substance use disorder, and a foundation that makes the rest of recovery possible.
Detox alone is not treatment for addiction. The National Institute on Drug Abuse describes medically managed withdrawal as a precursor to ongoing care, not a stand-alone solution.1 Detox stabilizes the body so that therapy, medication-assisted treatment, peer support, and relapse prevention work can begin in earnest.
The Substance Abuse and Mental Health Services Administration (SAMHSA) defines three goals for any detox program:
- Keep the patient safe at all times
- Treat withdrawal humanely with dignity and respect
- Prepare the person for entry into substance use treatment
A high-quality detox program does all three.
Who Needs Medical Detox?
Not every substance requires medically supervised withdrawal, but several do because their withdrawal syndromes can cause seizures, cardiac complications, severe dehydration, or psychiatric emergencies. Medical detox is strongly recommended when a person is physically dependent on alcohol, benzodiazepines, opioids, or barbiturates, or when several substances have been used together.
The American Society of Addiction Medicine (ASAM) Criteria are the clinical standard for matching a person to the right level of withdrawal management based on the substance involved, withdrawal severity, medical history, and co-occurring conditions.3 Anyone with a history of seizures, delirium tremens, heavy daily use, or a serious mental health condition should be evaluated for medical detox before attempting to stop.
- Alcohol. Heavy daily drinking can trigger alcohol withdrawal syndrome, including tremors, seizures, and life-threatening delirium tremens in severe cases.4
- Benzodiazepines. Stopping abruptly after long-term use can cause seizures and prolonged psychiatric symptoms; a slow medical taper is the standard of care.
- Opioids. Heroin, fentanyl, and prescription painkillers produce intense physical withdrawal that is rarely fatal in healthy adults but dangerously raises overdose risk if a person relapses.5
- Sedatives. Like benzodiazepines, abrupt cessation can cause seizures and require medical supervision.
- Stimulants. Cocaine, methamphetamine, and prescription stimulants do not usually cause life-threatening physical withdrawal, but the psychiatric symptoms (depression, suicidal thinking, severe fatigue) often warrant supervised care.

The Three Phases of Medical Detox
Most detox programs follow a three-phase model defined by SAMHSA: evaluation, stabilization, and transition to ongoing treatment.2 Each phase has a clinical purpose, and a quality program will be transparent about what happens at every step.
1. Evaluation
2. Stabilization
3. Treatment
Evaluation
The evaluation phase usually starts within hours of admission. Clinicians screen for substances in your blood and urine, take a full medical and psychiatric history, check vital signs, and may order lab work to look at liver function, electrolytes, and other markers. They use structured tools such as the Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) or the Clinical Opiate Withdrawal Scale (COWS) to track symptom severity.6
The output of evaluation is a personalized plan: which medications, how often vitals will be checked, what the level of care should be, and what to do if symptoms escalate.
Stabilization
Stabilization is the medical heart of detox. Nurses check vitals every few hours, score withdrawal symptoms on a regular schedule, and give medications to relieve discomfort and prevent complications. Hydration, nutrition, and sleep support are part of the plan. A psychiatrist or addiction medicine physician adjusts medications as withdrawal peaks and then tapers them as symptoms ease.
For most substances, the acute stabilization phase lasts 3 to 10 days, though longer stays are sometimes appropriate for benzodiazepines, alcohol with prior seizures, or polysubstance use.
Transition to Treatment
Detox without follow-up rarely leads to lasting recovery. SAMHSA describes the third phase as fostering patient readiness for and entry into treatment.2 A counselor reviews ongoing care options with you (inpatient rehab, partial hospitalization, intensive outpatient, or standard outpatient), arranges medication-assisted treatment if appropriate, and helps schedule admissions before discharge. This warm handoff is one of the strongest predictors of staying in care after detox ends.
Call A Treatment Provider
For a conversation about what treatment options are available to you.
Make a Call
Withdrawal Timelines by Substance
Detox timelines vary by substance, length of use, daily dose, individual physiology, and whether other drugs were involved. The table below summarizes typical acute withdrawal timelines reported in clinical literature.4,5,6
Many people also experience post-acute withdrawal syndrome (PAWS), which can include mood changes, sleep disturbance, and cravings for weeks or months after acute symptoms resolve.
| Substance | Onset of symptoms | Peak intensity | Acute phase ends | Notable risks |
|---|---|---|---|---|
| Alcohol | 6 to 24 hours after last drink | 24 to 72 hours | 5 to 7 days | Seizures, delirium tremens, dehydration |
| Short-acting opioids (heroin, oxycodone, fentanyl) | 8 to 24 hours | 36 to 72 hours | 5 to 10 days | Severe GI symptoms, dehydration, elevated overdose risk after detox |
| Long-acting opioids (methadone) | 24 to 48 hours | 3 to 8 days | 10 to 20 days | Prolonged discomfort, elevated overdose risk after detox |
| Short-acting benzodiazepines (alprazolam, lorazepam) | 6 to 24 hours | 2 to 4 days | 1 to 2 weeks, with taper | Seizures, severe anxiety, rebound insomnia |
| Long-acting benzodiazepines (diazepam, clonazepam) | 2 to 7 days | 5 to 14 days | 2 to 4 weeks, with taper | Seizures, prolonged psychiatric symptoms |
| Stimulants (cocaine, meth, amphetamines) | Hours after last use | 1 to 3 days | 1 to 2 weeks | Severe depression, suicidal ideation, exhaustion |
| Cannabis | 1 to 3 days | 2 to 6 days | 1 to 2 weeks | Irritability, sleep disturbance, appetite loss |

Medications Used in Medical Detox
Medications are the reason supervised detox is safer and more comfortable than going it alone. Clinicians use them in two ways: short-term medications that ease acute withdrawal symptoms, and longer-term medications that support relapse prevention after detox is complete.
The chart below shows the medications most often used in U.S. detox programs, organized by the substance being treated.
| Substance | First-line detox medications | What they do | Relapse prevention medications |
|---|---|---|---|
| Alcohol | Benzodiazepines (chlordiazepoxide, lorazepam, diazepam); anticonvulsants (gabapentin, phenobarbital) | Prevent seizures and delirium tremens, reduce autonomic symptoms, support sleep | Naltrexone, acamprosate, disulfiram |
| Opioids | Buprenorphine, methadone, clonidine, lofexidine | Suppress withdrawal symptoms, stabilize cravings, lower overdose risk after discharge | Buprenorphine (maintenance), methadone (maintenance), extended-release naltrexone |
| Benzodiazepines | Long-acting benzodiazepine taper (often diazepam); phenobarbital in select cases | Slow, controlled dose reduction to prevent seizures and rebound symptoms | No FDA-approved relapse medications; CBT and gradual dose tapers are standard |
| Stimulants | Supportive care; non-habit-forming medications for sleep, anxiety, and depression | Manage psychiatric and somatic symptoms during the crash | No FDA-approved relapse medications; behavioral therapies are first-line |
For people with opioid use disorder, medication-assisted treatment (MAT) with buprenorphine or methadone often begins during detox and continues as long as it is clinically helpful. Multiple federal agencies, including SAMHSA, treat MAT as the standard of care for opioid use disorder rather than an optional add-on.7

Inpatient vs. Outpatient Detox: Choosing the Right Setting
Medical detox can happen in several settings, ranging from a hospital intensive care unit to an outpatient clinic with daily visits. The right setting depends on the substance, withdrawal severity, medical and psychiatric history, and the stability of the person’s home environment. The ASAM Criteria describe five levels of withdrawal management; this section maps the two most common choices people actually face.3
| Inpatient (residential) detox | Outpatient detox | |
|---|---|---|
| Setting | Live at a detox facility or hospital; 24-hour nursing and physician access | Live at home; daily or near-daily clinic visits for monitoring and medication |
| Best for | Severe withdrawal, prior seizures or DTs, polysubstance use, co-occurring medical or psychiatric conditions, unstable home | Mild to moderate withdrawal, stable home, supportive sober family or roommates, no history of seizures |
| Typical duration | 3 to 10 days, sometimes longer | 1 to 2 weeks of clinic visits; medication taper may continue longer |
| Cost (out of pocket, before insurance) | $600 to $1,000+ per day on average | $250 to $500 per day on average |
| Advantages | Continuous monitoring, immediate medical response, removal from triggers | Lower cost, ability to keep working or caring for family, less disruption |
| Limitations | Higher cost, time away from work and family | Less supervision, exposure to triggers at home, not safe for severe withdrawal |
A clinical assessment is the only safe way to choose between the two. People often underestimate withdrawal risk, especially after years of heavy drinking or benzodiazepine use, and treating those at home can have serious consequences. If you are unsure which setting is appropriate, an admissions navigator at a treatment center or your primary care physician can run a brief screening over the phone.
Inpatient detox is often the front door to inpatient rehab, while outpatient detox commonly feeds into a partial hospitalization program or intensive outpatient program for continued treatment.
Does Insurance Cover Detox?
In most cases, yes. The Affordable Care Act classifies substance use disorder treatment, including detox, as an essential health benefit. That means Marketplace plans, Medicaid expansion plans, and most employer-sponsored plans are required to provide some level of coverage for medical detox.8 Medicare also covers medically necessary inpatient detox under Part A and outpatient detox services under Part B.
That said, “covered” does not always mean “free.” What you pay depends on several factors that vary plan by plan.
- In-network vs. out-of-network. In-network facilities have pre-negotiated rates and lower out-of-pocket costs. Out-of-network stays may not be covered at all on some plans.
- Medical necessity. Insurers often require documentation that inpatient detox is medically necessary based on withdrawal severity, prior seizures, or co-occurring conditions.
- Length-of-stay limits. Some plans approve detox in 3- to 5-day increments and require continued review for longer stays.
- Deductibles, copays, and coinsurance. Even with strong coverage, you may owe a percentage of the cost until you meet your out-of-pocket maximum for the year.
Before you commit to a facility, call your insurer or ask the treatment center’s admissions team to run a benefits check. Most treatment centers do this at no cost as part of admissions. For plan-specific guides covering large U.S. insurers, see our addiction treatment insurance hub.

How Much Does Medical Detox Cost?
Detox costs vary widely based on setting, length of stay, and which medications and services are included. Out-of-pocket prices look intimidating on paper, but insurance, sliding-scale facilities, and state-funded programs reduce what most people actually pay. The figures below represent typical published ranges before insurance is applied.
| Type of detox | Typical daily cost | Typical total cost (before insurance) |
|---|---|---|
| Outpatient medical detox | $250 to $500 per day | $1,000 to $3,500 for a typical course |
| Standard inpatient detox (free-standing center) | $600 to $1,000 per day | $1,800 to $7,000 for 3 to 7 days |
| Hospital-based or medically managed inpatient detox | $1,000 to $1,500+ per day | $5,000 to $10,000+ for 5 to 7 days |
| Executive or luxury detox programs | $1,500 to $2,500+ per day | $10,000 to $25,000+ for a 7-day stay |
Cost is one of the biggest reasons people delay treatment, but it is rarely the barrier it appears to be. For a detailed breakdown across all levels of care, see our guide to how much rehab costs.
Why At-Home Detox Can Be Dangerous
Quitting alcohol, benzodiazepines, or opioids without medical support is risky and, in some cases, life-threatening. SAMHSA and ASAM are explicit that self-detox is unsafe for alcohol or benzodiazepine dependence with a history of seizures, delirium tremens, or polysubstance use.2,3 Acute alcohol withdrawal alone has a fatality rate of up to 15% when severe cases go untreated, primarily due to DTs and seizures.4
Beyond the medical risk, at-home attempts often fail. Without medications to ease symptoms, cravings spike, and the urge to relapse is overwhelming. People who try to detox alone and relapse on opioids are at high risk of overdose because tolerance drops quickly during even brief abstinence.5

Detox Drinks, Kits, and Quick Fixes Do Not Work
Commercial detox drinks, herbal cleanses, and over-the-counter detox kits are marketed as fast ways to pass a drug test or speed up withdrawal. The Food and Drug Administration does not regulate most of these products, and there is no clinical evidence they treat physical dependence or reduce withdrawal symptoms.9 The only reliable way to detox is time, abstinence, and, when needed, medical support.

Rapid Detox
Equally cautious: programs that advertise “rapid” or anesthesia-assisted detox. These procedures compress opioid withdrawal under sedation, but carry serious cardiovascular and respiratory risks and have not been shown to improve long-term outcomes compared with standard detox.

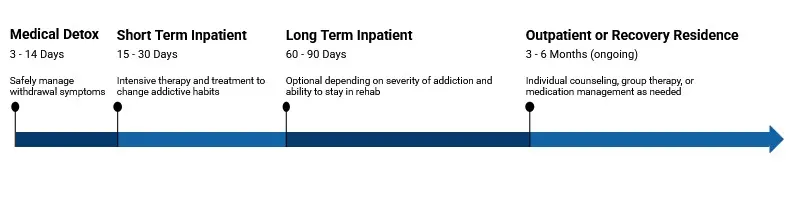
What Happens After Detox? The Continuum of Care
Detox stabilizes your body, but the work of recovery happens in the levels of care that follow. NIDA repeatedly emphasizes that brief detox alone produces poor long-term outcomes and should always be paired with ongoing treatment.1 Most people step down through the continuum below, sometimes spending time in two or three levels over the first year.
- Inpatient or residential rehab. 24-hour structured care, typically 30, 60, or 90 days, focused on therapy, skill-building, and stabilization.
- Partial hospitalization (PHP). Day treatment 5 to 6 days per week, with evenings at home or sober living.
- Intensive outpatient (IOP). Several group sessions per week, often 9 to 15 hours, while resuming work or school.
- Standard outpatient counseling. Weekly or biweekly therapy and medication management.
- Sober living homes and aftercare. Recovery housing, alumni programs, and ongoing peer support to extend gains made earlier.
Many people also continue medication-assisted treatment for months or years after detox, particularly for opioid and alcohol use disorders. Buprenorphine, methadone, naltrexone, and acamprosate have strong evidence for reducing relapse and overdose risk when used long-term.7

How to Choose a Detox Center
Not every detox program meets the same clinical standards. Before admitting yourself or a loved one, ask a short set of questions and verify the basics in writing or on the facility’s website.
- Licensing and accreditation. Confirm the center is licensed by its state and accredited by either The Joint Commission or CARF International. Accreditation signals that policies, staffing, and clinical procedures meet recognized standards.
- Medical staffing. A safe detox program has 24-hour nursing for inpatient care, a medical director with addiction medicine credentials, and access to a psychiatrist or psychiatric nurse practitioner for co-occurring conditions.
- Evidence-based medications. The program should follow current SAMHSA and ASAM guidance, including offering buprenorphine or methadone for opioid use disorder when clinically appropriate.
- Clear transition plan. Ask how they handle the move from detox into ongoing treatment. The best programs help schedule the next level of care before discharge.
- Insurance and financial transparency. A reputable facility will verify benefits up front, explain expected costs, and offer payment options or referrals if their program is not the right financial fit.
- Patient reviews and outcomes. Look at independent reviews and any published outcome data. Rehab.com’s Rehab Score combines reviews, brand reputation, accreditations, and other trust factors into a single quality signal.
If your loved one is resistant to treatment, a structured intervention with a trained professional can sometimes open the door to admission. And if you are not sure where to start, our guide to finding addiction treatment walks through the full decision process.
Frequently Asked Questions About Medical Detox
How long does medical detox take?
Most acute detox programs run 3 to 10 days, with alcohol and short-acting opioids on the shorter end and benzodiazepines or methadone often requiring longer tapers. Post-acute symptoms such as sleep disturbance and cravings can continue for weeks. Your length of stay is set by a clinician based on the substance, your medical history, and how your symptoms progress.
Is detox the same as rehab?
No. Detox is a short medical phase focused on clearing substances and managing withdrawal. Rehab is the longer treatment phase that follows, focused on therapy, skill-building, relapse prevention, and (when appropriate) medication-assisted treatment. NIDA and SAMHSA both treat detox as a precursor to rehab rather than a replacement for it.1,2
Can I work or stay with my family during detox?
Outpatient detox is sometimes appropriate for mild to moderate cases and allows people to live at home and continue working or caring for family. Inpatient detox requires a stay at the facility, usually for less than two weeks. A clinical assessment will determine which setting is safest for your situation.
Will I be in pain during detox?
Some discomfort is normal, but a properly run medical detox program uses medications and supportive care specifically to keep symptoms manageable. Opioid withdrawal in particular can feel like a severe flu, while alcohol and benzodiazepine withdrawal can involve anxiety, tremors, and insomnia. Medications such as buprenorphine, clonidine, and long-acting benzodiazepines significantly reduce symptom intensity.
What if I cannot afford detox?
Several options exist for people without insurance or with limited coverage. State-funded detox programs operate in every U.S. state through SAMHSA-funded networks, and many private facilities offer sliding-scale fees, payment plans, or scholarships. The SAMHSA National Helpline (1-800-662-HELP) is free, confidential, and available 24/7 to connect callers with local treatment options.10
Can I detox from multiple substances at once?
Yes, and polysubstance detox is one of the strongest reasons to choose inpatient over outpatient care. Combining alcohol or benzodiazepines with opioids or stimulants raises the medical complexity of withdrawal and the risk of complications. A medical team will sequence and dose medications carefully to manage each withdrawal syndrome at the same time.
Find Top Medical Detox Centers
Finding facilities near you…
Finding facilities near you…
Finding facilities near you…
References
- National Institute on Drug Abuse. Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition). National Institutes of Health. nida.nih.gov. Accessed June 2026.
- Substance Abuse and Mental Health Services Administration. TIP 45: Detoxification and Substance Abuse Treatment. SAMHSA. store.samhsa.gov. Accessed June 2026.
- American Society of Addiction Medicine. The ASAM Criteria, 4th Edition. ASAM. asam.org. Accessed June 2026.
- National Institute on Alcohol Abuse and Alcoholism. Alcohol Use Disorder: From Risk to Diagnosis to Recovery. NIAAA. niaaa.nih.gov. Accessed June 2026.
- Centers for Disease Control and Prevention. Opioid Overdose: Data and Trends. CDC National Center for Injury Prevention and Control. cdc.gov. Accessed June 2026.
- Sullivan JT, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: the revised Clinical Institute Withdrawal Assessment for Alcohol scale (CIWA-Ar). British Journal of Addiction. 1989;84(11):1353-1357. pubmed.ncbi.nlm.nih.gov. Accessed June 2026.
- Substance Abuse and Mental Health Services Administration. Medications for Substance Use Disorders. SAMHSA. samhsa.gov. Accessed June 2026.
- U.S. Department of Health and Human Services. Mental Health and Substance Use Disorder Coverage Under the Affordable Care Act. HHS. hhs.gov. Accessed June 2026.
- U.S. Food and Drug Administration. Beware of Products Promising Miracle Weight Loss and Detox Claims. FDA Consumer Updates. fda.gov. Accessed June 2026.
- Substance Abuse and Mental Health Services Administration. National Helpline (1-800-662-HELP). SAMHSA. samhsa.gov. Accessed June 2026.





