
































































































The ASAM Levels of Care for drug rehab and addiction treatment are established by The American Society of Addiction Medicine (ASAM). People trying to understand more about standardized recovery services across the United States and access these programs use this guide to compare plans when seeking treatment.
This guide explains each level of care and why the distinctions matter, how placement decisions are made, and how people move between levels throughout the treatment process. The most recent edition of the ASAM Criteria (the Fourth Edition, released in 2023)3 introduced several updates to how levels of care are defined and organized, and this guide reflects those changes.
Levels of Care: Key Facts
- ASAM Levels of Care create a common clinical language for addiction treatment across the United States.
- Each level describes a different intensity of support, from early intervention (Level 0.5) to medically managed inpatient care (Level 4).
- Placement is determined through a structured assessment across six clinical dimensions, not by a single factor such as substance type or severity alone.
- The ASAM Fourth Edition (2023) added Level 1.0 Long-Term Remission Monitoring and formally recognized Recovery Residences as a distinct support tier.
- Movement between levels, called stepping up or stepping down, is a planned part of treatment, not a sign of failure.
- Insurance coverage for each level is governed by medical necessity criteria that closely follow the ASAM framework.
In This Article:
- What are Levels of Care in Addiction Treatment?
- Choosing Level of Care
- Level 4: Medically Managed Intensive Inpatient (Medical Detox)
- Level 3: Residential & Inpatient Rehab
- Level 2: Intensive Outpatient & Partial Hospitalization
- Level 1: Standard Outpatient Treatment
- Level 0: Intervention and Aftercare
- Moving Through the Continuum: Step Up & Step Down Care
- Supportive Services That Span All Levels
- Special Populations & Tailored Considerations
- Paying for Treatment & Navigating Insurance
- Frequently Asked Questions About Levels of Care
- Find Treatment Near You
What are Levels of Care in Addiction Treatment?
The ASAM defines five broad levels of addiction treatment, ranging from outpatient therapy to medically managed inpatient care. Each level reflects a different intensity of clinical support, matched to a person’s assessed needs across six dimensions of health and life circumstances. A person can move between levels throughout treatment as their recovery progresses.
The American Society of Addiction Medicine created a framework called the ASAM Criteria to give providers and treatment-seekers a consistent way to determine the right intensity of care. The framework is the most widely used set of placement standards in the United States and is used by treatment programs, insurance companies, and state Medicaid agencies to guide clinical decisions.
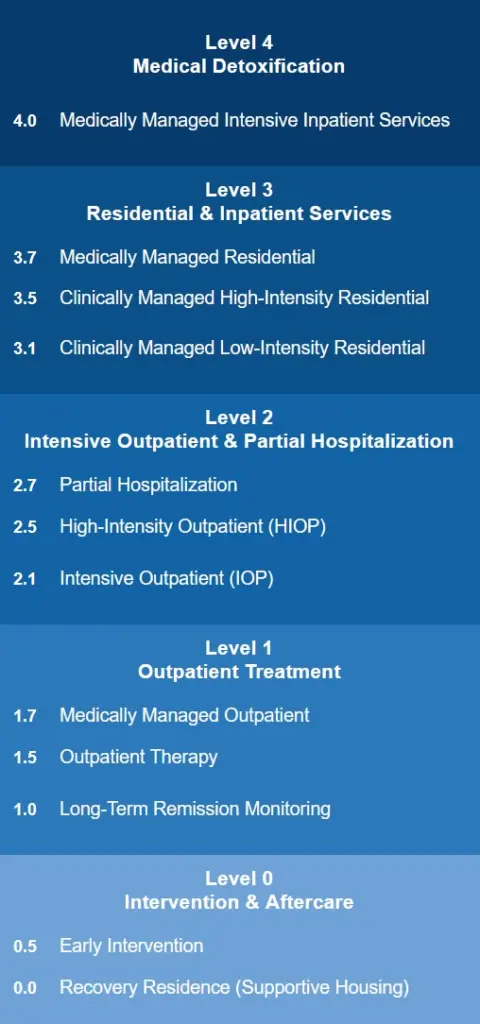
The ASAM system includes five broad levels of care, numbered 0 through 4, with decimal sub-levels indicating further gradations of intensity:
- Level 4 is the highest level of care and consists of medically managed inpatient rehab treatment, typically in a hospital or specialized unit.
- Level 3 involves clinically managed residential care, where a person lives at the treatment facility.
- Level 2 care is provided through partial hospitalization or intensive outpatient programs, which provide structured daily treatment without overnight stays.
- Level 1 is standard outpatient care including therapy and telehealth, involving fewer than nine hours of programming per week.
- Level 0.5 addresses early intervention for people who show signs of problematic use but do not yet have a diagnosed substance use disorder.
Aftercare, sober living, and long-term remission monitoring sit at the lower end of the continuum and support people who have completed active treatment.
How Is Level of Care Determined?
Clinicians use the ASAM Criteria to evaluate a person across six dimensions of health and life circumstances, including withdrawal risk, mental health, and living environment. The results guide placement into the least intensive level of care that is still safe and effective. This assessment happens at intake and is repeated regularly to guide transitions throughout treatment.
When someone seeks addiction treatment, the first step is a structured clinical assessment using the ASAM Criteria. This evaluation looks at six areas of a person’s life, called dimensions, that together inform the appropriate level of care.
The assessment does not rely on a single factor like substance type or frequency of use. A clinician reviews all six dimensions and recommends the least intensive level of care that can safely meet that person’s needs.
| Level of care | Who is this for | Average daily cost | Medical supervision | Length of stay | Time required |
|---|---|---|---|---|---|
| Medical detox | Severe withdrawal, high-risk cases | $500 to $1,000 | 24/7 medical staff | 3 to 14 days | Full-day monitoring |
| Inpatient | Co-occurring disorders, chronic use | $300 to $800 | 24/7 clinical support | 30 to 90 days | Full-day, live-in |
| Intensive outpatient | Employed, stable home, relapse risk | $100 to $300 | Limited, non-medical | 8 to 12 weeks | 3 to 5 hours/day, 3 to 5 days/week |
| Outpatient | Mild use, early-stage recovery | $50 to $150 | Minimal or none | Varies, often ongoing | 1 to 2 hours/week or as needed |
The six ASAM dimensions are:
- Acute intoxication and withdrawal potential: Is the person currently intoxicated, and what is their risk of withdrawal complications?
- Biomedical conditions and complications: Are there physical health conditions that affect treatment or require medical management?
- Emotional, behavioral, and cognitive conditions: Are there mental health symptoms, psychiatric diagnoses, or cognitive impairments that need to be addressed alongside addiction?
- Readiness to change: In the Fourth Edition, this dimension is integrated across all other dimensions rather than scored separately. It influences the services offered at each level of care.
- Relapse, continued use, or continued problem potential: How likely is the person to return to use without structured support?
- Recovery and living environment: Does the person have stable housing, supportive relationships, and access to care? This dimension was updated in the 2023 Fourth Edition to explicitly include social determinants of health (SDOH) and barriers to care.
The assessment results are applied to the ASAM Dimensional Admission Criteria to generate a recommended level of care.
Treatment programs at Levels 3.1, 3.5, and 3.7 can obtain ASAM Level of Care Certification through CARF International, which independently verifies that a program can deliver care consistent with ASAM standards.1,3

Level 4: Medically Managed Intensive Inpatient (Medical Detox)
Level 4 is the most intensive care setting, providing 24-hour medical supervision in a hospital or specialized unit. It is appropriate when a person faces significant withdrawal risk or requires medical stabilization before other treatment can begin. Most people transition to a lower level of care such as residential or intensive outpatient treatment once they are medically stable.
Level 4 care is indicated when a person has significant withdrawal symptoms, is at risk of severe or complicated withdrawal, or requires medical stabilization for another reason. Medically assisted detox is provided while substances are safely cleared from the body under the supervision of a medical team that typically includes nurses and medical and mental health clinicians.
Level 4 interventions are commonly used for acute alcohol withdrawal and opioid use disorder. Medications such as benzodiazepines and anticonvulsants may be used to manage withdrawal symptoms including anxiety, insomnia, and seizure risk. These medications can also prevent delirium tremens in people with severe alcohol dependence.
Care takes place in a hospital or a residential rehab center with a dedicated medical unit, and is available around the clock. Inpatient detox typically lasts up to 10 days. Once medically stable, most people transition to a residential or intensive outpatient program, where the focus shifts to counseling and behavioral treatment.

Level 3: Residential & Inpatient Rehab
Level 3 consists of residential drug rehab programs where a person lives at the facility while receiving structured addiction care. Programs range from high-intensity therapeutic communities (Level 3.5) to low-intensity residential settings (Level 3.1), depending on assessed needs. Unlike Level 4, Level 3 does not require around-the-clock physician-managed medical care.
All inpatient programs provide addiction counseling, relapse prevention education, food, and housing. The specific clinical intensity varies by sub-level.
Level 3.7 Medically Monitored Inpatient / Detox
For individuals who require after hours monitoring or robust support level 3.7 provides access to biomedical services for managing subacute detox, withdrawal symptoms, pregnancy, wounds, IV medications, infections and relapse and mental health risks.
This medically managed level includes physician daily rounds, onsite nurses and psychiatric care. It functions as the critical bridge between hospital detox and residential rehab.
Level 3.5 High Intensity Therapeutic Community
Level 3.5 is suited for individuals with severe behavioral and social functional impairments who can benefit from highly structured settings and 24 hour support.
They can access mild withdrawal symptoms support and peer supervision to prevent substance use. Psychosocial counseling for navigating interpersonal interactions and fulfilling daily responsibilities alongside life and recovery-sustaining skills are available to promote long-lasting behavior change.
Level 3.3 Medium Intensity (Long Term Care)
Level 3.3 was removed from the latest version (4th edition) of the ASAM criteria in 2023.
These long term programs ran longer than 90 days and helped individuals with cognitive impairments address chronic relapse patterns by tailoring slow paced interventions that incorporated vocational training and community responsibilities.
ASAM’s updated treatment criteria include slow-paced modalities in all levels to embed care for individuals with cognitive deficits within each stage of recovery.
Level 3.1 Low Intensity Residential
Level 3.1 helps individuals with moderate risks of substance use and have unstable home environments to benefit from 24 hour residential support and structure.
Patients access assistance for managing daily routines, develop skills to better function in society, participate in peer support and relapse-prevention activities and receive counseling while attending work or school part time.

Level 2: Intensive Outpatient & Partial Hospitalization
Level 2 includes partial hospitalization programs (PHP) and intensive outpatient programs (IOP), both of which provide structured treatment without overnight stays. PHP involves 20 or more hours of programming per week and is suited to people with complex needs or those stepping down from residential care. IOP offers 9 to 20 hours per week for those with mild to moderate addiction who can maintain stability at home.
People who step down from Level 3 typically enter Level 2 outpatient care. Both PHP and IOP provide multiple hours of structured clinical programming each week while allowing people to return home at night.
Partial Hospitalization Programs (Level 2.7)
A partial hospitalization program (PHP) or day program provides drug rehab treatment for 20+ hours per week through outpatient services that take place for 4 to 6 hours a day on 3 or more days a week. There are no overnight stays even though PHP treatment is provided as an option at some residential rehab facilities.
Programs typically last for a minimum of 30 days and cost about $11,000 to $13,000 per month. PHP treatment usually includes individual and group counseling, addiction and relapse prevention education and often treatment for co-occurring mental health disorders.

Intensive Outpatient Programs (Levels 2.1 & 2.5)
An intensive outpatient program (IOP) typically provides 9 to 20 hours of treatment per week over 2 or 3 days. Sessions usually last 3 to 6 hours per day.
IOP is a popular choice among people who’ve mild to moderate addiction and who aren’t at risk for withdrawal complications. The recommended duration for IOP treatment is 90 days.
IOP can be used as an entry point to rehab treatment or as a stepdown program following inpatient or residential treatment. The cost for IOP is around $15,000 to $20,000 for a 3 month program.

Level 1: Outpatient Treatment
Level 1 is standard outpatient treatment, involving fewer than nine hours of programming per week in a clinic or practitioner’s office. It is designed for people with mild addiction or those stepping down from more intensive care. Telehealth addiction services, available via phone or video, are also categorized at this level.
Outpatient Treatment (Levels 1.5 and 1.7)
Outpatient treatment is best suited for people with less severe addiction symptoms and low risk of significant withdrawal.
Sessions take place in a freestanding clinic or a provider’s office, for fewer than nine hours per week spread over one to three sessions. Program lengths typically range from 28 days to six months, with three months being most common.
Research shows that inpatient treatment is associated with greater abstinence in the first month after discharge. At the six-month mark, outcomes for people in outpatient and inpatient treatment tend to converge for those who remain engaged in care.4

Long-Term Remission Monitoring (Level 1.0)
The ASAM Criteria Fourth Edition (2023)3 added Level 1.0 as a formal tier for people who have achieved sustained remission but benefit from ongoing monitoring and rapid re-engagement support. This level includes scheduled check-ins, recovery management services, and structured pathways to step back into active treatment if needed.
Level 1.0 reflects a chronic-care model of addiction treatment, one that recognizes recovery as an ongoing process rather than a fixed-duration course of care. It is analogous to the ongoing monitoring that people with other chronic conditions, such as diabetes or hypertension, receive from their care teams even during periods of stability.
Online Rehab & Telehealth
Telehealth for addiction treatment offers care remotely through an internet video connection or a phone call. This format has become widely used since the COVID-19 pandemic and remains widely available. Both individual and group sessions can be attended via telehealth.
Telehealth tends to be more affordable than in-person visits and removes transportation as a barrier, which is particularly valuable for people in areas where treatment centers are scarce.
Potential limitations include challenges with technology access and the absence of a structured physical environment that some people find helpful in early recovery.

Level 0: Early Intervention and Sober Living
Level 0 covers two distinct parts of the care continuum: early intervention for people at risk of developing a substance use disorder, and recovery residences for people who have completed formal treatment.
Both focus on prevention, relapse prevention, and sustained community support rather than active clinical treatment. Neither requires 24-hour care or structured programming.
Level 0.5: Early Intervention Services
Early intervention at Level 0.5 addresses people who are using substances in harmful ways but do not yet meet diagnostic criteria for a substance use disorder. The goal is to reduce substance use and prevent escalation before a more serious disorder develops.
Common settings for early intervention include primary care offices, employee assistance programs (EAPs), school-based programs, and emergency departments.
Services typically involve brief motivational counseling, education about substance use risks, and connection to community resources. Because these interactions are brief and low-barrier, they can reach people who would not otherwise seek treatment.
Research consistently shows that addressing substance misuse before a diagnosable disorder develops produces better long-term outcomes and reduces the cost of future care. SAMHSA’s Screening, Brief Intervention, and Referral to Treatment (SBIRT) model is among the most widely used early intervention frameworks in the United States.
Level 0.0: Recovery Residence & Sober Living
Sober living homes are also considered aftercare on the ASAM continuum. These are residences shared by multiple individuals in the process of recovery after they have completed their treatment programs.
These facilities are an inexpensive option for those who want to maintain social connections and share mutual accountability with others who also desire to maintain a sober lifestyle.
A sober home typically has a house manager who assigns household chores and enforces drug free environment rules. Some sober homes hold 12 Step meetings onsite, which have been shown to have positive effects on residents’ ongoing sobriety.
Rent in sober homes is the responsibility of the resident but government assistance and grants are often available.

Stepping Up and Stepping Down in Treatment
Movement between levels of care is a planned, clinical process, not a sign of failure. When a person’s needs change, their care team reassesses and adjusts accordingly, either stepping down to less intensive care as recovery progresses or stepping up to more intensive support when symptoms worsen or relapse occurs. Reassessments happen regularly throughout treatment.
Stepping down refers to transitioning from a more intensive level of care to a less intensive one as a person stabilizes and gains recovery skills. A common step-down pathway looks like this: medical detox (Level 4) to residential treatment (Level 3) to partial hospitalization (Level 2.7) to intensive outpatient (Level 2.1) to standard outpatient (Level 1) to continuing care and peer support.
Not everyone follows this sequence from the top. Many people enter treatment at Level 2 or Level 1, particularly those with mild to moderate addiction and stable living situations. Step-down planning begins during the intake assessment and is updated throughout treatment.
The ASAM Criteria include specific continued-service and transfer criteria that guide these decisions. Level-of-care changes are made on clinical grounds, not based on how long a person has been in a given program or whether their insurance has covered a fixed number of days.
Typical Treatment Timeline
According to ASAM’s criteria each person moves along the continuum of care based on how they respond to treatments. There are no predetermined lengths of stay at any level.
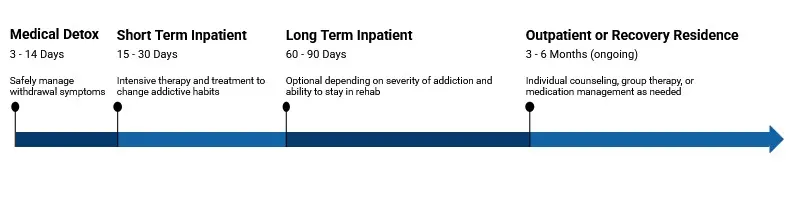
A person may stay five days in a Level 4 program while detoxing, then transition to a 30 day Level 3 program to address the underlying reasons for substance abuse. Then they may enroll in an 8 week intensive outpatient treatment program (IOP) to develop life skills. After IOP they could join an outpatient program for continuous support.
Each stage of the healing journey embeds prevention strategies throughout to promote lasting recovery.
Warning Signs You May Need to Step Back Up
Addiction’s chronic nature means that relapse is always a possibility. If a person in a Level 2 program develops uncontrollable drug cravings, misses counseling sessions or tests positive in drug screens these warning signs could indicate a need for a reassessment of the level of care needed.
The Recovery Capital Index (RCI) is used by medical professionals to periodically evaluate a client’s progress along the continuum of care. If the warning signs suggest the client requires additional support the RCI can be used to decide to step back on a level to reroute therapeutic progress.
Crafting a Relapse Prevention & Aftercare Plan
With adequate tools and support it’s possible to implement practical relapse prevention and aftercare strategies. For example, establishing SMART goals and signing recovery contracts can increase personal commitment to sobriety.
Accessing a crisis phone tree can offer practical support during a crisis.
Regular follow up appointments and alumni events can foster connections and instill hope. A graduate understands that care continues even after a program has formally ended. This encourages individuals to remain committed to progress within a sober community.
Services That Span All Levels
In all programs the care team may require selected services to enhance the rehab experience. Since everyone’s conditions are unique programs like methadone maintenance or counseling to address certain mental conditions may be warranted to strengthen recovery.
Of U.S. adults with a substance use disorder, 44% also live with a co-occurring mental health condition (SAMHSA 2023 NSDUH).
Of the 48.5 million U.S. adults with a substance use disorder in 2023, 85.4% did not receive any substance use treatment (SAMHSA 2023 NSDUH).
Medication Assisted Treatment
Sometimes medication assisted treatment (MAT) that uses a special group of FDA-approved prescriptions is necessary to ease strong withdrawal symptoms or cravings.
FDA approved methadone, buprenorphine and naltrexone can alleviate these urges in someone with opioid use disorder. Naltrexone, acamprosate and disulfiram are MAT options for alcohol use disorder.
MAT generally begins during or shortly after medical detox in the first treatment stage. Its use, response and adherence are monitored at various ASAM Levels of Care as a person progresses throughout the healing continuum as their withdrawal slowly subsides.

Dual-Diagnosis & Psychiatric Care
Approximately 56% of American adults with addictions also have mental health conditions.2 That’s why addressing co-occurring disorders is embedded in every level of the ASAM criteria
Mental health status can rapidly change as treatment advances. Tackling dual diagnoses with integrated mental-health meds and counseling can reduce relapse rates, while screening for PTSD, depression and ADHD early in recovery results in more robust treatments for addressing the underlying reasons for substance abuse.

Family Therapy, Peer Coaching, & Holistic Treatment
Programs such as Community Reinforcement and Family Training (CRAFT) and multidimensional family therapy (MDFT) engage the families and loved ones of adults and adolescents who are battling addiction.
They strengthen communication skills, increase problem-solving capabilities and teach family members how to help and be a source of encouragement. Peer coaches can increase treatment retention by fostering accountability and personal commitment.
Tools like alumni apps for check-ins are also valuable aids to promote a sense of community and dedication to sustained recovery.
Aftercare Programs
Addiction treatment aftercare encompasses the support a person receives after completing formal treatment. Aftercare is a non-numbered level of care on the ASAM continuum that reflects the modern understanding of addiction as a chronic condition where recurrence is possible and care reinitiation could be necessary.
Effective aftercare typically includes some combination of the following:
- Ongoing individual or group therapy
- Continued medication-assisted treatment (MAT) for opioid or alcohol use disorder
- Participation in peer support groups such as Alcoholics Anonymous or SMART Recovery
- Transitional housing arrangements
There’s usually no cost for alumni meetings and events. Depending on the severity of addiction and the level of care program graduates may attend aftercare for more than a year.
Special Populations & Tailored Considerations
The ASAM Levels of Care can guide treatment, but physicians understand that programs must be customized to suit their patients. Specific demographic groups defined by age, gender and occupation may require specialized methodologies within their level of care.
1 in 15 Veterans
About 1 in 15 U.S. veterans had a substance use disorder in the past year, with rates higher among post-9/11 veterans (SAMHSA NSDUH).
Priority Access
Pregnant clients receive priority placement in publicly funded substance use treatment in most states, with care coordinated across OB/GYN, addiction medicine, and pediatrics (SAMHSA).

Adolescents vs. Adults
Adolescents have unique recovery needs compared to adults. Adolescents’ brains are developing while they battle substance abuse. They face challenges like family dynamics, trauma, peer pressure and school stress that demand specialized recovery approaches.
Family-centric care, school coordination and experiential therapies that factor in adolescents’ shorter attention spans can aid recovery.
The ASAM is working on a new version (fourth edition) of the Adolescent and Transition Age Youth volume to update best practices to help young lives recover.

Pregnant Clients & Neonatal Concerns
Pregnant clients with addictions are often given priority access in the continuum of care due to the harm alcohol or drug abuse can pose to unborn children.
Medication-assisted treatment is often the initial step to safely quit and reduce fetal stress. Clinicians monitor the mothers 24/7 to watch for complications and adjust the doses accordingly.
In addition, addiction can affect the capacity of pregnant women to take care of themselves. Coordination with OB/GYN, pediatric and social services is prioritized to incorporate prenatal care as part of a holistic recovery approach.
Veterans, Chronic Pain & Trauma-Informed Care
Trauma informed care is a central tenet of the ASAM criteria because trauma is strongly associated with elevated substance use.
Veteran-specific peer groups offer a military friendly environment where recovery addresses moral injury, which is a common effect of combat. These services help veterans reframe PTSD triggers with tools like eye movement desensitization and reprocessing (EMDR) therapy to break patterns that may influence addiction.
Integrated pain management is also a critical component of recovery programs. Chronic pain can result in seeking relief through addictive substances.

LGBTQ+ Affirmative Programming
The LGBTQ+ community has unique challenges that affect how they access recovery services. Issues like trauma, stigma, discrimination and isolation are all better addressed in safe spaces specifically designed to help minorities cope with stress.
Affirmative services include trained staff on pronouns, gender appropriate housing and counseling for underlying mental health conditions. Programs take place within environments that emphasize privacy to encourage comfortable disclosure and sustainable healing.

Paying for Treatment & Navigating Insurance
The cost of treatment varies and depends on the level of care, amenities, types of services, location and many individual factors.
Cost averages for main level of care are:
- Detox: Between $250 and $1000 per day depending on services and inpatient or outpatient alternatives.
- Inpatient/residential: 30 day programs cost between $6,000 to $25,000 depending on facilities, amenities and location. 60 to 90 day treatment ranges from $10,000 up to $60 to 80K.
- Partial hospitalization: These less intensive programs average between $5,000 to $20,000.
- Outpatient: These programs on average cost $1,000 to $2,000 per month with more luxurious facilities charging $3,000 or more monthly.
It’s critical to understand that most insurers cover recovery programs. To decide what to cover, most payers utilize ASAM levels as the clinical benchmark to evaluate what constitutes a medical necessity and what doesn’t.
When a person seeks help to recover a qualified professional utilizes the ASAM dimensions of addiction as decision-making parameters to assess an individual’s medical needs. The professional then generates a formal requirement via signed letters and a proposed treatment plan for insurers’ approval.

Financing, Scholarships & State-Funded Options
If you’re uninsured, there are still alternatives to explore. Most rehab facilities offer sliding scale plans, scholarships and financial aid options worth considering.
Based on your circumstances you may qualify for state and nonprofit-financed rehab centers, employee assistance programs (EAP), SAMHSA block grants, specialty court vouchers and other financial alternatives.
Overcoming addiction can be the most valuable investment you ever make for yours and your family’s future.

Frequently Asked Questions About Levels of Care
The questions below address the most common points of confusion about how addiction treatment levels work, how placement is determined, and what to expect when moving between levels of care.
Detox: 3 – 7 days
Residential program: 4 – 12 weeks
IOP: 6 – 12 weeks
Outpatient: 12+ weeks
The exact timeframe of each level varies from person to person and is dependent on treatment response, not predetermined lengths.
You can work or attend school while accessing IOP and OP programs that feature flexible scheduling that adjusts to your circumstances. A PHP requires a 4 to 6 hours daily commitment 5/days a week so you’ll need to rearrange your schedule to make it work. Residential programs may demand a full-time commitment to recovery.
Yes. Insurance covers all levels of treatment as parity law requires that mental health and substance use treatment cannot have less coverage than other types of treatments if they’re deemed a medical necessity. Coverage varies depending on insurance plans and the specific medical needs of each individual.
Sober-living homes are considered Level 0 supportive environment post-treatment by the ASAM criteria. They aren’t an active form of substance abuse treatment but can supplement the recovery journey as sources of stable living conditions for individuals who’ve participated in evidence based programs and may lack a safe place to live.
A trained clinician determines the appropriate level of care through a structured ASAM assessment covering six dimensions of health and life circumstances. The assessment results guide placement into the least intensive level of care that is still safe and effective. You cannot self-assign a level of care, but understanding the framework can help you ask better questions during intake.
Partial hospitalization (PHP) provides 20 or more hours of structured treatment per week, while intensive outpatient (IOP) typically involves 9 to 20 hours per week. PHP is appropriate for people with complex clinical needs or those stepping down from residential care. IOP is better suited for people who can maintain daily stability at home while attending regular treatment sessions.
Yes, if a clinician determines that the person is not at risk for severe or complicated withdrawal. A person with mild to moderate alcohol or opioid use may safely begin outpatient treatment without detox. When withdrawal risk is present, medically supervised detox is always the recommended starting point before other treatment begins.
A relapse is a clinical event that triggers reassessment, not a reason to discharge someone from care. The clinical team will reassess the person’s needs across the six ASAM dimensions to determine whether the current level of care is still appropriate or whether stepping up to a more intensive setting would better support recovery.
Find Treatment Near You
With over 22,000 rehab centers listed Rehab.com’s rehab center directory is the most comprehensive solution to find a recovery facility that adapts to your preferences and budget. We screen all facilities on various quality metrics to help you make an informed decision.
You can filter by location, level of care, insurance and special programs to see the top ranked centers in your city or state based on our proprietary rehab scoring methodology.
Not sure where to start? Call the number below to talk with someone who’ll assist you in finding the best treatment options based on your insurance coverage and unique needs.
Call A Treatment Provider
For a conversation about what treatment options are available to you.
Make a Call
Featured Rehab Centers
Finding facilities near you…
Resources
- CARF International. Commission on Accreditation of Rehabilitation Facilities. Published 2024. Accessed April 1, 2026. https://carf.org/
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2023 National Survey on Drug Use and Health. HHS Publication No. PEP24-07-021, NSDUH Series H-59. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration; 2024. https://www.samhsa.gov/data/report/2023-nsduh-annual-national-report
- American Society of Addiction Medicine. The ASAM Criteria, Fourth Edition. Rockville, MD: American Society of Addiction Medicine; 2023. https://www.asam.org/asam-criteria
- National Institute on Drug Abuse. Principles of Drug Addiction Treatment: A Research-Based Guide. 3rd ed. Bethesda, MD: National Institute on Drug Abuse, National Institutes of Health; 2018. https://nida.nih.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition





