
































































































Drug and Alcohol Addiction: What It Is, Why It Happens, and How to Get Help
In 2024, an estimated 48.4 million people in the United States aged 12 or older met the clinical criteria for a substance use disorder.¹ If you are searching for answers about your own use or someone you care about, you are not alone, and this page is a place to start.
What follows is a direct explanation of what addiction actually is, what is happening in the brain, the signs that distinguish casual use from a clinical disorder, what raises risk, and what effective treatment looks like.
Key Points
- Substance use disorder (SUD) is a chronic brain disease, not a moral failing or a lack of willpower. The DSM-5 classifies it on a spectrum from mild to severe.
- Addiction develops through repeated exposure that gradually rewires the brain’s reward, stress, and decision-making circuits. Two people with similar use histories can end up in very different places.
- Genetics account for roughly 40 to 60 percent of individual risk, but environment, trauma, and the age use begins are equally important.
- More than 45 percent of adults with a substance use disorder also have a mental health condition. Treating only one without the other rarely works.
- Treatment is effective, available, and usually covered by insurance. Earlier intervention leads to better outcomes, and recovery does not require hitting a crisis point.
In This Article:
- What is drug and alcohol addiction?
- How does addiction develop?
- How addiction affects the brain
- Signs and symptoms of drug and alcohol addiction
- What causes addiction? Risk factors and vulnerability
- Types of drug and alcohol addiction
- Addiction and mental health
- How addiction affects families
- Common myths about drug and alcohol addiction
- When is it time to get help?
- What does addiction treatment involve?
- Frequently asked questions
- References
What is drug and alcohol addiction?
Drug and alcohol addiction, clinically called substance use disorder (SUD), is a chronic medical condition in which a person continues to seek and use a substance despite serious harm to their health, relationships, or daily functioning. The American Psychiatric Association, the National Institute on Drug Abuse (NIDA), and the Substance Abuse and Mental Health Services Administration (SAMHSA) all classify SUD as a brain disease.² ³ It is not a character flaw or a failure of willpower.
Addiction exists on a spectrum. The Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) rates its severity as mild, moderate, or severe based on the number of diagnostic criteria a person meets. “Addiction” in everyday language generally refers to the moderate-to-severe end of that spectrum, where use has become compulsive and where stopping (even when a person wants to) is genuinely difficult.
Alcohol use disorder (AUD) is the most common form of SUD in the United States, followed by cannabis use disorder and opioid use disorder.¹ Any substance that produces changes in the brain’s reward system carries some risk of disordered use. SUD also commonly occurs alongside mental health conditions, because the two share overlapping brain pathways and each can worsen the other.
80% of people in the U.S. who needed treatment for a substance use disorder in 2024 did not receive it.¹
Roughly 46% of adults with a substance use disorder also have a co-occurring mental illness.¹
Use, misuse, dependence, and addiction
One of the most common sources of confusion in this topic is the difference between substance use, misuse, tolerance, physical dependence, and addiction. These terms are often used interchangeably, but they describe different conditions, and the distinctions matter for treatment.
Use is the act of consuming a substance. Misuse is using a substance outside its intended purpose, such as taking a higher dose of a prescription painkiller than prescribed, or drinking heavily on a regular basis. Misuse increases risk, but it is not the same as having a clinical disorder.
Tolerance and physical dependence are biological adaptations. Tolerance means a person needs more of a substance to achieve the same effect; physical dependence means the body has adjusted to the substance enough that stopping triggers withdrawal symptoms. Both can occur with medications that a doctor prescribed for a legitimate medical reason. A person taking long-term opioids for chronic pain, for example, may develop tolerance and physical dependence without having an addiction.³
Addiction is a behavioral pattern that adds compulsive use and continued use despite clear harm. It is possible to have addiction without significant physical dependence (for example, with cocaine or methamphetamine), and it is possible to have physical dependence without addiction (for example, with a medically supervised antidepressant or a prescribed opioid taken as directed).
| Concept | What it means | Who can have it |
|---|---|---|
| Tolerance | Needing more of a substance to feel the same effect. | Anyone who uses a substance regularly, including patients on prescribed medications. |
| Physical dependence | The body has adapted to the substance; stopping triggers withdrawal symptoms. | Common with opioids, benzodiazepines, alcohol, and some other prescribed medications, with or without addiction. |
| Misuse | Using a substance in a way it was not intended (higher dose, more often, recreationally, or someone else’s prescription). | Anyone, often with no clinical disorder yet. |
| Substance use disorder (SUD) | A clinical condition diagnosed via DSM-5 criteria. Compulsive use and continued use despite harm. Spectrum: mild, moderate, severe. | Diagnosed by a clinician based on number of criteria met in the past 12 months. |
| Addiction | Everyday term for moderate-to-severe SUD. Compulsive use plus loss of control plus continued use despite consequences. | People meeting four or more DSM-5 criteria for a substance use disorder. |
Why this matters in practice: a person tapering off a prescribed benzodiazepine after years of medical use may experience genuine withdrawal without having an addiction. Treatment is a medical taper, not a rehab admission.
A person whose use has crossed into compulsive cocaine use may have severe addiction without dramatic physical withdrawal. Treatment is behavioral therapy, structured care, and sometimes medication.
Getting the diagnosis right shapes the entire treatment plan.
How does addiction develop?
Drug and alcohol addiction rarely appears overnight. It progresses through stages, and because the shift between stages can be gradual, many people do not recognize a problem until it is well established. Researchers and clinicians commonly describe four stages of use that precede a clinical diagnosis.⁴
- Experimental or prescribed use: A person tries a substance for the first time, often in a social context, or begins taking a prescribed medication as directed. There is no pattern yet, only an initial exposure.
- Regular use: Use becomes more frequent. Social or recreational use settles into a pattern. The substance is incorporated into specific situations such as weekends, social events, or after work. Tolerance has not necessarily developed.
- Harmful or heavy use: Use is routine. Days off become rare. Tolerance develops, so a person needs more of the substance to feel the same effect. Negative consequences begin to appear, but use continues. This stage is often called problematic use or substance misuse.
- Substance use disorder: Use is daily or near-daily. The person has lost meaningful control over the amount or frequency, and attempts to cut back repeatedly fail. The DSM-5 diagnostic threshold is reached, and severity ranges from mild to severe.⁴
Most people do not move through these stages on a fixed timeline. Genetics, mental health, the substance itself, and how often a person uses it all influence how quickly someone progresses. Opioids and methamphetamine, for example, can lead to clinical disorder in weeks for some users. Alcohol or cannabis use often takes years to escalate to that level for others.⁵
The progression is also not always one-directional. Some people move backward through stages on their own, especially earlier in the trajectory. Others stay in heavy use for years without meeting the diagnostic threshold. What distinguishes addiction from heavy use is the loss of control and the continued use despite known harm, both of which are observable through clinical criteria rather than amount alone.
Call A Treatment Provider
For a conversation about what treatment options are available to you.
Make a Call
How addiction affects the brain
Addiction is best understood as a brain disease, which is to say that the changes occurring inside someone with a substance use disorder are not metaphorical. They are visible on imaging, measurable through neurochemistry, and consistent across substances.
When someone uses alcohol or drugs, the brain’s reward system releases a surge of dopamine, a chemical that signals pleasure and motivates repeated behavior. This is a normal mechanism; it is how the brain reinforces eating, social connection, and other behaviors important for survival. Substances exploit that same system, producing dopamine releases far larger than any natural reward.⁵
Over time, the brain responds to those artificial surges by reducing its own dopamine production and the sensitivity of dopamine receptors. The result is that ordinary pleasures feel flat and the substance starts to feel necessary just to feel normal. This is why cravings feel urgent, why stopping is physically and psychologically painful, and why relapse can happen years after a person has stopped using.
The prefrontal cortex, the brain region responsible for decision-making and impulse control, is also affected by sustained heavy use. This helps explain why a person with a substance use disorder may continue to use even when they clearly recognize the costs. The brain’s control mechanisms have been compromised by the very substance causing the harm.⁵
Recovery allows the brain to rebalance, but the process takes time. Longer treatment durations and sustained support work in part because they give the brain the substance-free period it needs to begin healing. Imaging studies show that the brain can show partial recovery within months of abstinence, with further structural and functional improvements continuing over a year or more in many people.⁵
The three stages of the addiction cycle
Researchers have developed a three-stage model that describes how addiction maintains itself in the brain over time. This framework, sometimes called the Koob-Volkow model, is the basis for the U.S. Surgeon General’s neurobiological description of addiction in Facing Addiction in America.¹¹
The three stages do not happen once and stop. They form a cycle that repeats, and as the cycle repeats, each stage tends to intensify. Different brain regions and neurotransmitter systems are involved at each stage, which is why no single medication or therapy targets all of them.
1. Binge / Intoxication
The substance is consumed and the brain’s reward circuits flood with dopamine. The basal ganglia drive the pleasurable, reinforcing effects that keep a person coming back. Over time, the reward feels less intense, so the person uses more.¹¹
2. Withdrawal / Negative Affect
When the substance leaves the body, the extended amygdala produces stress, anxiety, irritability, and physical symptoms. The person now uses to escape feeling bad rather than to feel good. This is negative reinforcement, and it strengthens the cycle.¹¹
3. Preoccupation / Anticipation
Between episodes, the prefrontal cortex struggles to override cravings. Decision-making and impulse control weaken. A trigger such as a place, a person, or a mood reactivates anticipation of use, and the cycle restarts. This is where most relapses begin.¹¹
One useful implication: cravings and relapse risk in early recovery are not signs of weak commitment. They are predictable features of a brain that is still cycling through stage three. Evidence-based treatments such as cognitive behavioral therapy, relapse prevention, and medication-assisted treatment work in part by giving the prefrontal cortex tools to interrupt that cycle while the brain rebuilds.
Signs and symptoms of drug and alcohol addiction
There is no single sign that confirms a substance use disorder. Clinicians make that determination by applying the DSM-5 criteria. But the warning signs that often prompt a person or family to seek a clinical assessment tend to follow recognizable patterns across four areas: behavioral, physical, psychological, and social.
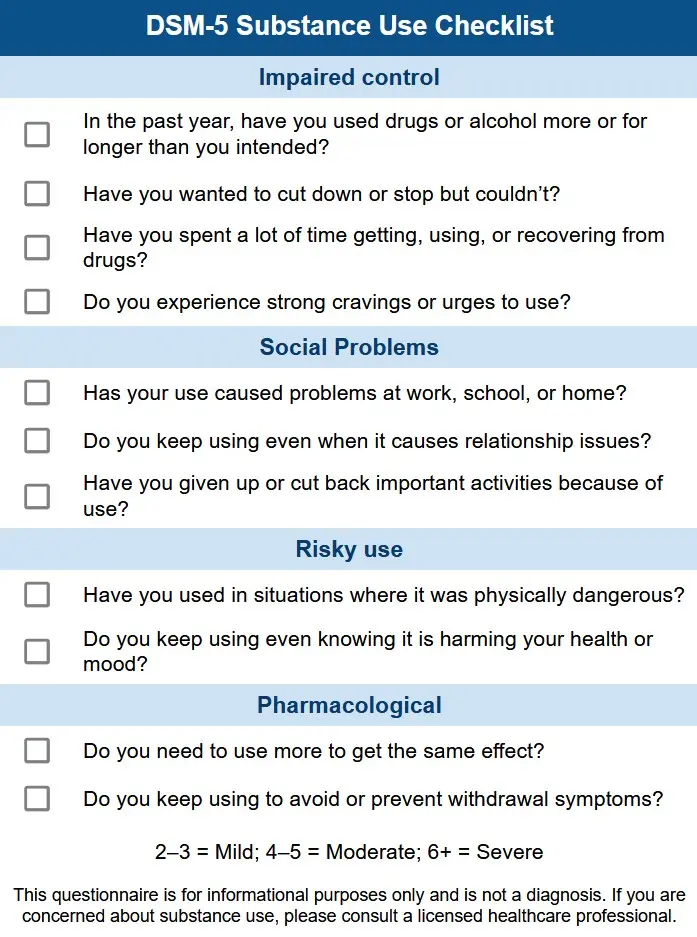
DSM-5 criteria: how clinicians diagnose substance use disorder
The DSM-5 identifies 11 diagnostic criteria for substance use disorder.⁶ A clinician evaluating someone for SUD looks at how many of the following applied in the previous 12 months.
Loss of control
- Using more of the substance, or for longer, than intended
- Repeated unsuccessful efforts to cut down or stop
- Spending a great deal of time obtaining, using, or recovering from the substance
- Experiencing persistent cravings or strong urges to use
Social and role impairment
- Failing to meet obligations at work, school, or home because of substance use
- Continuing to use despite persistent or recurring problems in relationships caused or worsened by use
- Giving up social, occupational, or recreational activities in order to use
Risky use
- Using in situations where doing so creates physical risk (such as driving)
- Continuing to use despite a known physical or psychological problem that is caused or worsened by the substance
Physical changes
- Tolerance: needing noticeably more of the substance to achieve the same effect
- Withdrawal: experiencing characteristic symptoms when use is reduced or stopped
Two to three criteria in 12 months indicates mild SUD. Four to five indicates moderate. Six or more indicates severe.⁶
Warning signs in a loved one
Most family members and friends do not have DSM-5 criteria in mind when they begin to worry about someone. What they notice is a pattern of changes. These do not prove a substance use disorder on their own, but in combination they are reasons to seek a professional assessment.
| Category | What you may notice |
|---|---|
| Behavioral | Secrecy about whereabouts or activities; new social group; loss of interest in hobbies; deteriorating performance at work or school; unexplained absences; lying about use or money. |
| Physical | Significant weight loss or gain; declining personal hygiene; bloodshot eyes; changes in sleep patterns; tremors, shakes, or slurred speech; track marks or unexplained injuries; frequent illness. |
| Psychological / mood | Mood swings, irritability, or unexplained anger; increased anxiety or paranoia; emotional flatness; depressive symptoms; appearing intoxicated, withdrawn, or absent in conversation. |
| Social and financial | Borrowing or stealing money; missing items in the home; avoiding family events; relationship conflict; trouble keeping a job; legal problems related to use such as a DUI. |
Signs look different from person to person and substance to substance. Someone with alcohol use disorder may show mainly behavioral changes such as missed obligations, relationship conflict, and irritability when sober. Someone with opioid use disorder may show more physical markers such as withdrawal symptoms, changed sleep, and significant weight loss. If you are concerned about your own use or a loved one’s, a clinical assessment is the most reliable path to an accurate picture.
What causes addiction? Risk factors and vulnerability
No single factor explains why one person develops a substance use disorder while another with similar exposure does not. Research consistently identifies three categories of risk, and they interact with one another rather than acting in isolation.
Biology and genetics
Genetics account for approximately 40 to 60 percent of individual vulnerability to addiction, according to NIDA.⁵ Having a parent or sibling with a SUD raises statistical risk without determining outcomes. Variations in genes that regulate dopamine signaling and the stress response are among the biological mechanisms researchers have identified, and twin studies confirm the heritable component across nicotine, alcohol, opioid, and stimulant use disorders.
Environment
Early exposure to substances, trauma, chronic stress, childhood neglect or abuse, and easy access to drugs or alcohol all increase risk. Adverse childhood experiences (ACEs), including physical or emotional abuse, household substance use, and parental mental illness, have a measurable, cumulative relationship with the likelihood of later addiction.⁷ Limited access to mental health care and housing or economic instability also raise vulnerability.
Developmental timing
The earlier someone begins using a substance, the higher their risk. The adolescent brain is more susceptible to the rewiring effects of repeated substance exposure than the adult brain. People who begin using substances before age 18 are four to seven times more likely to develop a SUD than those who start in adulthood.⁵
40 to 60%
Of individual addiction risk is attributable to genetics, according to NIDA.
4 to 7x Higher Risk
Of developing a substance use disorder for those who begin using before age 18, compared to adult-onset use.
Risk factors are not destiny. Protective factors such as stable family relationships, mental health support, strong social connection, and delayed onset of use meaningfully reduce risk even when biological or environmental vulnerabilities are present. Two siblings with the same genetic and family environment can have very different trajectories depending on age of first use, the substances they encounter, and the support systems around them.
Types of drug and alcohol addiction
Substance use disorders can develop with almost any psychoactive substance. The most prevalent in the United States include alcohol, cannabis, opioids, stimulants, benzodiazepines, hallucinogens, and behavioral addictions such as gambling. Each has a distinct profile of effects, withdrawal patterns, and treatment considerations, but the underlying neurobiology is similar.
| Substance category | Estimated U.S. prevalence (2024) | Key notes |
|---|---|---|
| Alcohol use disorder (AUD) | ~28 million adults¹ | Most common SUD. Withdrawal can be medically dangerous and often requires supervised detox. |
| Cannabis use disorder | ~19 million people aged 12+¹ | Rising with higher-THC products. Treatment is primarily behavioral. |
| Opioid use disorder (OUD) | ~5.7 million people aged 12+¹ | Includes prescription opioids, heroin, and fentanyl. Highly responsive to MAT. |
| Stimulant use disorder (cocaine, methamphetamine, prescription stimulants) | ~4.5 million combined people aged 12+¹ | No FDA-approved medication; behavioral therapy is the primary treatment. |
| Sedative, hypnotic, or anxiolytic use disorder (benzodiazepines, sleep medications) | ~1.4 million people aged 12+¹ | Withdrawal can be medically dangerous; tapering must be supervised. |
| Hallucinogen use disorder | Less than 1 million people aged 12+¹ | Less common; treatment is largely behavioral and supportive. |
| Behavioral addictions (gambling disorder is the most studied) | ~2.5 million U.S. adults estimated to meet criteria for gambling disorder¹² | No substance involved, but the same reward circuitry is engaged. |
Polysubstance use, the use of more than one substance at the same time, is increasingly common and significantly raises medical risk. The CDC reports that overdose deaths involving multiple drugs continue to climb even as overall overdose deaths have begun to decline.⁸ Combining alcohol with benzodiazepines or opioids, or using stimulants and opioids together, sharply increases the risk of respiratory failure and overdose.

Addiction and mental health
More than 45 percent of adults with a substance use disorder also have a co-occurring mental health condition, and the overlap is even higher (47 percent) among adults with serious mental illness.¹ The most common pairings involve depression, anxiety disorders, PTSD, bipolar disorder, and ADHD, though any psychiatric condition can co-occur with SUD.
The relationship runs in both directions. Mental health conditions increase the risk of developing a SUD, often because substances temporarily relieve distressing symptoms. This pattern is a documented pathway into disordered use for many people. At the same time, sustained heavy use of alcohol or drugs can trigger or worsen depression, anxiety, psychosis, and other psychiatric conditions. By the time someone enters treatment, it is often difficult to establish which came first.

Clinicians use the term dual diagnosis to describe the combination. Treating only the substance use while leaving a mental health condition unaddressed (or vice versa) significantly reduces the likelihood of sustained recovery.⁹ Integrated treatment that addresses both conditions at the same time is the standard of evidence-based care, and most accredited rehab programs are equipped to provide it.
Our dual diagnosis guide covers co-occurring conditions in detail, including depression and addiction, anxiety and alcohol or drug use, PTSD and substance use disorder, bipolar disorder, and ADHD.
How addiction affects families
Addiction rarely stays contained to the person experiencing it. Partners, children, parents, and close friends are drawn into its effects, often carrying financial strain, emotional exhaustion, and relational damage that accumulates quietly over years.
Family members commonly develop responses to a loved one’s addiction that, over time, can make it easier for use to continue. Covering for missed responsibilities, providing money that goes toward substances, or consistently avoiding conflict around use are examples of enabling patterns.
These are rarely intentional. Most family members are trying to manage a crisis with whatever tools they have available. Understanding where support ends and enabling begins is one of the most useful things a family member can learn.
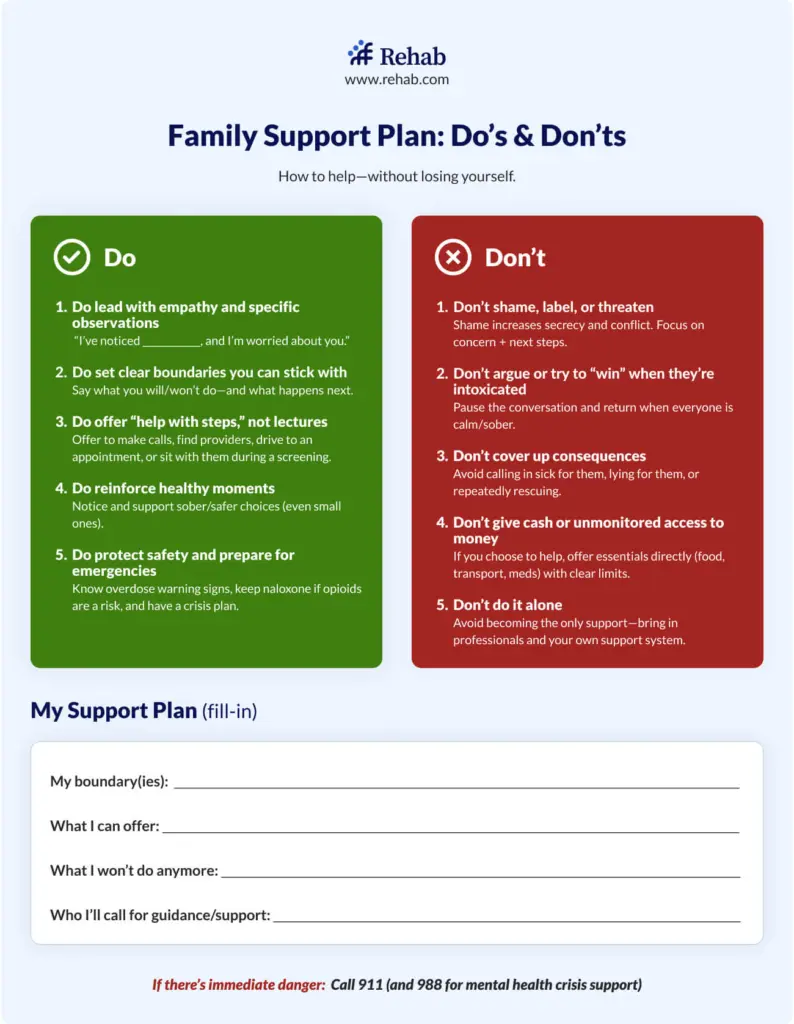
When a family member is unwilling to seek help on their own, a structured intervention, typically facilitated by a trained interventionist, can provide a focused opportunity for family and friends to express concern and present a concrete treatment option. See our guides on how addiction affects families and how to stage an intervention.
Common myths about drug and alcohol addiction
Stigma is one of the most consistent barriers to treatment. Many of the most common beliefs about addiction are inconsistent with the clinical evidence, and they keep people from seeking care that would otherwise help them.¹⁰ The table below addresses the ones our editorial team hears most often from readers and family members.
| Myth | What the evidence shows |
|---|---|
| Addiction is a choice or a failure of willpower. | The first decision to use a substance is voluntary. Addiction is not. Repeated exposure produces measurable changes in the brain’s reward, stress, and decision-making circuits that compromise the ability to stop, even when a person clearly wants to.² ⁵ |
| A person has to hit “rock bottom” before treatment can work. | Treatment is more effective the earlier it begins. Waiting for a crisis costs years, relationships, and in many cases, lives. There is no severity threshold a person needs to cross to deserve care.¹⁰ |
| Prescription medications are safe by definition. | Opioids, benzodiazepines, and prescription stimulants all carry addiction risk even when taken as prescribed, particularly with long-term use. Risk varies by substance, dose, duration, and individual vulnerability. |
| Relapse means treatment has failed. | Relapse is a recognized feature of a chronic medical condition, the same way symptom recurrence is common in diabetes, hypertension, or asthma. Long-term outcomes improve with continued treatment, not with the assumption that one episode of care should be enough.¹⁰ |
| Medication-assisted treatment (MAT) just trades one addiction for another. | FDA-approved medications such as methadone, buprenorphine, and naltrexone stabilize brain chemistry and significantly reduce overdose risk. The medical and scientific consensus, including the American Society of Addiction Medicine, treats MAT as evidence-based care, not as a continued addiction.² |
| Addiction only happens to certain kinds of people. | Substance use disorders occur across every demographic, income level, education level, and profession. Genetics, environment, mental health, and developmental timing influence risk, but no group is exempt. |
| If a person really wanted to stop, they could. | The compulsive use and inability to stop are diagnostic features of the disorder. Recovery typically requires a combination of medical treatment, therapy, and ongoing support, the same multimodal approach used for other chronic conditions. |
Misinformation about addiction is not harmless. SAMHSA estimates that more than half of adults who needed treatment in recent years cited cost, lack of information about where to go, or fear of being judged among their reasons for not seeking care.¹ Replacing the willpower model with the clinical model is a meaningful part of closing that gap.
When is it time to get help?
If substance use is affecting your health, your relationships, your work, or your ability to function, and you have found it genuinely difficult to cut back on your own, that pattern is worth taking seriously with professional support.
Many people delay seeking help for years, often because they believe their situation is not severe enough, or that they should manage it without outside assistance. Substance use disorder is a medical condition. The expected response to a chronic medical condition is clinical support, and the evidence is consistent: earlier intervention leads to better outcomes.¹⁰ A person does not need to reach a crisis point to deserve care.
If you are ready to take a next step, the options are broader than most people expect. Treatment includes flexible outpatient programs built around work and family responsibilities, short-term inpatient stays, and medication-assisted treatment that substantially reduces cravings and withdrawal. Cost and insurance are common concerns; under the Affordable Care Act, most major insurance plans are required to cover substance use disorder treatment. See our insurance for rehab guide for help verifying your coverage.
Call A Treatment Provider
For a conversation about what treatment options are available to you.
Make a Call
What does addiction treatment involve?
Effective treatment addresses more than substance use in isolation. The most widely supported approaches combine medical care, behavioral therapy, peer support, and attention to underlying mental health conditions.
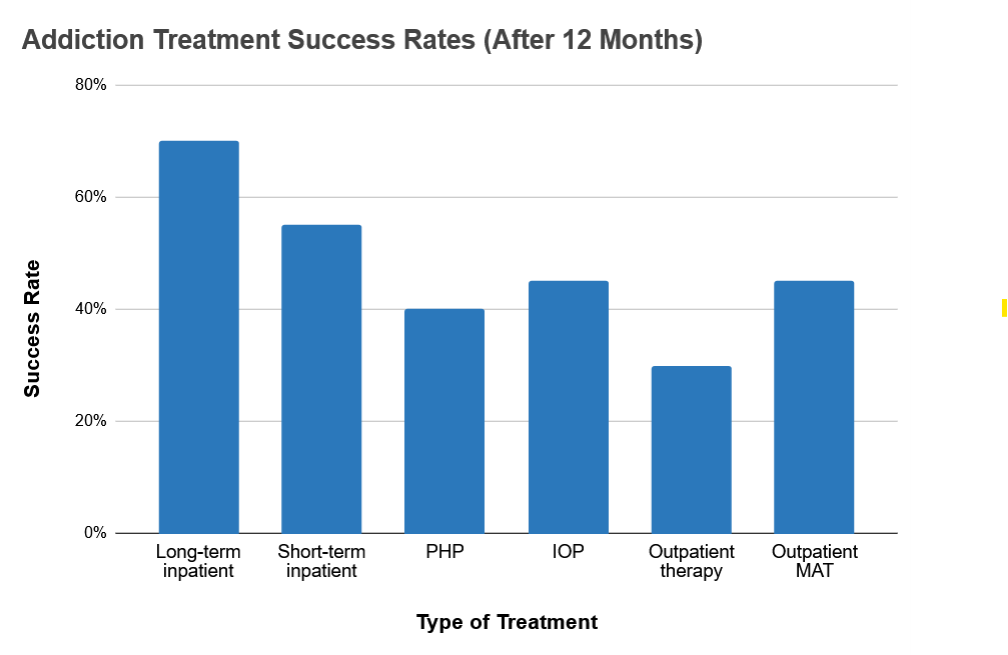
The standard continuum of care, defined by the American Society of Addiction Medicine, includes several levels. The appropriate starting point depends on the severity of the SUD and the person’s circumstances.

Medical detox
Medical detox is the supervised management of withdrawal, with medications to reduce discomfort and prevent dangerous complications. Detox is the necessary first step for people with significant physical dependence on alcohol, opioids, or benzodiazepines. It is not treatment on its own, but it makes treatment possible.
Inpatient and residential rehab
Inpatient or residential treatment provides 24-hour structured care, typically lasting 30, 60, or 90 days. It is the appropriate level for people with severe SUD, an unstable home environment, co-occurring medical needs, or prior treatment attempts that have not held.
PHP and IOP
Partial hospitalization (PHP) and intensive outpatient (IOP) are structured day programs that allow a person to return home in the evenings. PHP and IOP are common step-down options after residential care, and the primary route for many people who cannot take extended time away from work or family.
Standard outpatient
Standard outpatient involves weekly or twice-weekly therapy sessions. Appropriate for mild-to-moderate SUD with a stable home environment, and a common maintenance level after completing higher levels of care.
Medication-assisted treatment (MAT)
Medication-assisted treatment (MAT) uses FDA-approved medications to reduce cravings and withdrawal for opioid and alcohol use disorders. Methadone, buprenorphine (Suboxone), and naltrexone (Vivitrol) are among the most studied. MAT is a medical treatment that supports neurological stabilization while a person rebuilds their life, not a substitute addiction.
Aftercare and support groups
Aftercare and ongoing peer support are critical for long-term recovery. Options include sober living homes, ongoing therapy, and peer-support groups such as Alcoholics Anonymous, Narcotics Anonymous, and SMART Recovery. Recovery is a long-term process, and structured support during the first year or two of abstinence significantly improves outcomes.
Specialty programs
Specialty programs are available for specific populations, including veterans, adolescents, LGBTQ+ individuals, women, men, and working professionals and executives. These programs adapt the evidence-based core of addiction treatment to the specific needs and circumstances of the populations they serve.
Frequently asked questions
Is addiction a disease?
Yes. NIDA, the American Society of Addiction Medicine (ASAM), the American Psychiatric Association, and the World Health Organization all classify addiction as a chronic brain disease. It produces measurable changes in brain structure and function, it has identifiable genetic and environmental risk factors, and it responds to medical treatment. Describing addiction as a moral failure is inconsistent with the clinical evidence and is one of the factors that prevents people from seeking care.²
What is the difference between physical dependence and addiction?
Physical dependence occurs when the body adapts to a substance such that reducing or stopping use causes withdrawal symptoms. A person can be physically dependent on a medication a doctor prescribed without having a substance use disorder. Addiction (moderate-to-severe SUD) adds the component of compulsive use and continued use despite clear harm. Both conditions can coexist, but dependence alone does not equal addiction.³
Is addiction genetic?
Genetics play a significant role. NIDA estimates they account for 40 to 60 percent of individual risk.⁵ Having a family history of addiction raises statistical vulnerability without making a substance use disorder inevitable. Environmental factors, developmental timing, and mental health all interact with that genetic risk, and protective factors can reduce it meaningfully.
Can someone recover from addiction?
Yes. Millions of people in the United States are in sustained recovery from addiction. SAMHSA reports that of the 67.8 million U.S. adults who say they have ever had a mental health or substance use issue, roughly 67 percent consider themselves to be in recovery or to have recovered.¹ Recovery looks different from person to person. Some reach it through inpatient treatment, others through outpatient therapy and medication, others through peer support. Relapse is common and does not mean treatment has failed; it is a recognized feature of a chronic condition.
How long does it take to become addicted?
There is no fixed timeline. Some people develop a SUD after a relatively brief period of heavy use, particularly with substances that carry high addiction potential such as opioids or methamphetamine. Others use for years without meeting the clinical criteria for a disorder. Individual biology, genetics, mental health, and the substance itself all affect how quickly disordered patterns develop. Early, frequent, or heavy use accelerates risk across all substance categories.⁵
Is overdose still rising in the United States?
Overdose deaths declined sharply in 2024. The CDC reports 79,384 drug overdose deaths in 2024, down roughly 27 percent from 2023 and the lowest annual total since 2019.⁸ Most of the decline came from a drop in synthetic opioid (largely fentanyl) deaths. Methamphetamine-involved overdose deaths increased over the same period, and overdose remains the leading cause of death among Americans aged 18 to 44. Experts attribute the decline to expanded access to naloxone, increased availability of medication-assisted treatment, and shifts in the illicit drug supply.
Will my insurance cover addiction treatment?
Most major insurance plans are required to cover substance use disorder treatment under the Affordable Care Act. Specific benefits, copays, in-network providers, and prior authorization requirements vary by plan. Our insurance for rehab guide walks through how to verify your benefits, and our cost of rehab guide outlines typical out-of-pocket ranges by level of care.
Find Addiction Treatment Centers
Finding facilities near you…
Finding facilities near you…
Finding facilities near you…
References
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2024 National Survey on Drug Use and Health. HHS Publication No. PEP25-07-021. Rockville, MD: SAMHSA; 2025. https://www.samhsa.gov/data/data-we-collect/nsduh-national-survey-drug-use-and-health/national-releases/2024. Accessed June 2026.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Publishing; 2013.
- National Institute on Drug Abuse. Understanding Drug Use and Addiction DrugFacts. Published January 2023. https://nida.nih.gov/publications/drugfacts/understanding-drug-use-addiction. Accessed June 2026.
- Cleveland Clinic. Substance Use Disorder (SUD). Updated November 2025. https://my.clevelandclinic.org/health/diseases/16652-drug-addiction-substance-use-disorder-sud. Accessed June 2026.
- National Institute on Drug Abuse. Drugs, Brains, and Behavior: The Science of Addiction. Updated April 2020. https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction. Accessed June 2026.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5). Washington, DC: American Psychiatric Publishing; 2013:490-491.
- Centers for Disease Control and Prevention. About Adverse Childhood Experiences. Updated 2024. https://www.cdc.gov/aces/about/index.html. Accessed June 2026.
- Centers for Disease Control and Prevention, National Center for Health Statistics. Drug Overdose Deaths in the United States, 2023-2024. NCHS Data Brief No. 549. Hyattsville, MD: NCHS; 2025. https://www.cdc.gov/nchs/products/databriefs/db549.htm. Accessed June 2026.
- Substance Abuse and Mental Health Services Administration. Co-occurring Disorders and Other Health Conditions. Updated 2023. https://www.samhsa.gov/co-occurring-disorders. Accessed June 2026.
- McLellan AT, Lewis DC, O’Brien CP, Kleber HD. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA. 2000;284(13):1689-1695. doi:10.1001/jama.284.13.1689
- U.S. Department of Health and Human Services, Office of the Surgeon General. Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health. Chapter 2: The Neurobiology of Substance Use, Misuse, and Addiction. Washington, DC: HHS; 2016. https://www.ncbi.nlm.nih.gov/books/NBK424849/. Accessed June 2026.
- National Council on Problem Gambling. Problem Gambling FAQ. Updated 2024. https://www.ncpgambling.org/help-treatment/faq/. Accessed June 2026.





