
































































































Drug and alcohol addictions are significant problems in the U.S. According to the Substance Abuse and Mental Health Services Administration, 48.7 million Americans ages 12 and older had a substance use disorder in the past year, but fewer than 25% received any treatment.1
If you are trying to understand your options, this page covers the full range of treatment choices for drug and alcohol addiction and how to match the right one to your situation.
Key points
- Addiction treatment is not a single program. It is a continuum that ranges from residential care to outpatient therapy and peer support.
- The right level of care depends on the substance involved, addiction severity, the presence of co-occurring conditions, and home environment stability.
- Medication-assisted treatment (MAT) is an evidence-based option for opioid and alcohol use disorders.
- Most major insurance plans are required under the Affordable Care Act to cover substance use disorder treatment.
- Aftercare planning is a critical part of effective treatment, not an optional add-on.
- A quality treatment program will be licensed by its state, accredited by a recognized body, and use evidence-based approaches.
In This Article:
- Is addiction treatable?
- Levels of care explained
- How to choose the right level of care
- Online and telehealth addiction treatment
- Medication-assisted treatment (MAT)
- Therapy and behavioral treatment
- Treating co-occurring mental health conditions
- Specialty treatment programs
- Support groups and peer recovery
- How much does addiction treatment cost?
- What to look for in a treatment center
- What happens after treatment?
- Treatment FAQs
Is addiction treatable?
Yes. The National Institute on Drug Abuse (NIDA), the American Society of Addiction Medicine (ASAM), and SAMHSA all classify addiction as a treatable chronic disease. Research shows that most people who enter treatment and remain in it stop or substantially reduce their drug and alcohol use, reduce criminal activity where applicable, and improve their occupational, social, and psychological functioning.2
No single treatment approach works for everyone. Effective treatment is matched to an individual’s clinical needs, addresses more than substance use in isolation, and adjusts over time as those needs change. NIDA identifies 13 principles of effective drug addiction treatment, which form the scientific basis for what “evidence-based” means in a clinical addiction context.
Among the most important: treatment does not need to be voluntary to be effective, and behavioral therapy combined with medication where applicable produces the best outcomes for most people.2
If you are still asking whether a problem exists, our drug and alcohol addiction guide covers the signs, causes, and nature of addiction in detail before you think about treatment options.
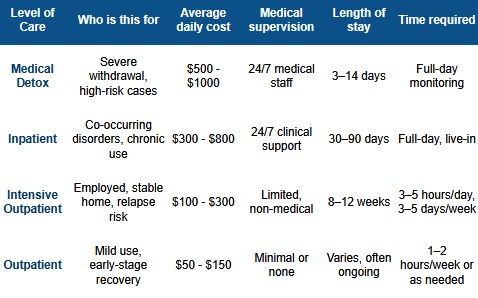
The treatment continuum: levels of care explained
Addiction treatment is not a single program. It is a continuum with different levels of intensity matched to different stages of severity and recovery. The American Society of Addiction Medicine defines this continuum from early intervention through medically managed intensive inpatient care.3
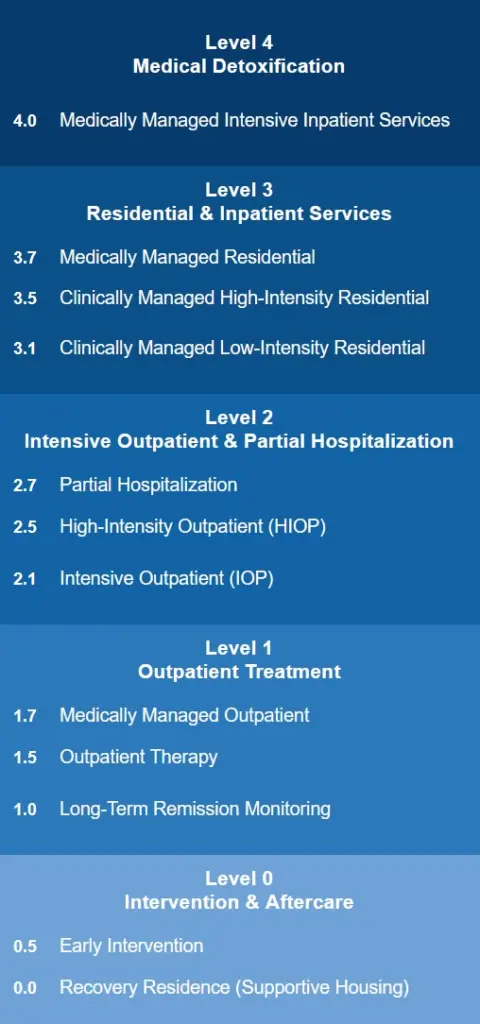
Most people move through multiple levels during a full course of treatment, stepping down in intensity as they stabilize.

The levels below run from highest to lowest intensity.
Medical detox
Medical detox is the supervised management of withdrawal. People who have developed physical dependence on alcohol, opioids, benzodiazepines, or other substances can experience severe and in some cases life-threatening withdrawal symptoms when they stop, including nausea, uncontrollable shaking, agitation, seizures, and delirium. Medical detox allows a person to clear substances from their body safely while under around-the-clock clinical supervision.
Medical detox programs are typically led by a physician and include nursing staff, clinicians, and mental health professionals trained in addiction medicine. Depending on the withdrawal presentation, physicians may prescribe medications including methadone, buprenorphine, benzodiazepines, or other agents to reduce symptoms and prevent complications.
The average detox process lasts seven to ten days, though this varies based on the substance, frequency and duration of use, quantity used, and individual factors including body chemistry, metabolic rate, and overall health.4 Detox typically takes place at a dedicated medical detox center, a hospital, or as part of an inpatient program.
One important distinction: detox by itself is not addiction treatment. It safely manages the acute physical phase of withdrawal. Once a person has medically stabilized, comprehensive treatment begins.

Inpatient and residential treatment
Inpatient drug rehab provides 24-hour structured care in a residential setting. Patients live on-site while receiving continuous medical support and a comprehensive treatment program that addresses both the physical and psychological dimensions of addiction. This generally includes a combination of individual therapy, group therapy, family and couples counseling, holistic therapies such as meditation and mindfulness, relapse prevention training, and trauma-focused care where applicable.
The average stay at an inpatient treatment center is 28 days. NIDA research indicates that treatment longer than 90 days is associated with more positive outcomes in many cases.2 A key practical advantage of inpatient care is that it removes a person from the environments, people, and stressors associated with their use, allowing them to be fully present in the recovery process.
Inpatient treatment is most appropriate for people with severe SUD, significant physical withdrawal risk, a co-occurring medical or psychiatric condition that requires close monitoring, an unstable home environment, or prior attempts at outpatient treatment that did not hold.

Partial hospitalization (PHP)
Partial hospitalization programs provide a high level of clinical structure comparable to inpatient care, but on a day-treatment basis. Patients attend programming for at least 20 hours per week and return to home or sober living in the evenings. PHP is appropriate for people who need psychiatric and medical support alongside addiction treatment but do not require 24-hour inpatient residence. It is a common step-down from inpatient care.

Intensive outpatient (IOP)
Intensive outpatient programs provide structured group and individual therapy, typically requiring at least nine to fifteen hours of participation per week. IOP allows people to continue working, attending school, and managing family responsibilities while receiving a meaningful level of clinical support. Programs commonly include trauma education, relapse prevention, vocational skills, emotional regulation, and group therapy.
IOP is appropriate as a primary treatment level for people with moderate SUD and a stable, supportive home environment. It is also a widely used step-down option after inpatient or PHP. Research consistently shows that treatment lasting a minimum of 90 days is associated with better outcomes, regardless of the setting.2

Standard outpatient
Standard outpatient addiction treatment involves one to two therapy sessions per week. It is appropriate for people with mild-to-moderate SUD who have a stable home environment and a reliable support system. Outpatient treatment is also the most common maintenance level of care for people who have completed a more intensive program.
Because outpatient care does not isolate a person from their environment, it is generally not recommended as the primary treatment for people in early recovery with severe SUD or significant environmental risk factors.

Sober living and recovery residences
Sober living homes provide structured, substance-free housing as a bridge between inpatient treatment and independent living. Residents return to daily activities such as work, school, and community involvement while living in a peer-supported, accountable environment. As of 2020, there were an estimated 17,000 recovery residences in the United States, with residents staying for an average of seven months.5 Supervision levels vary: some homes are peer-run with minimal monitoring, while others have credentialed staff and more formal programming.

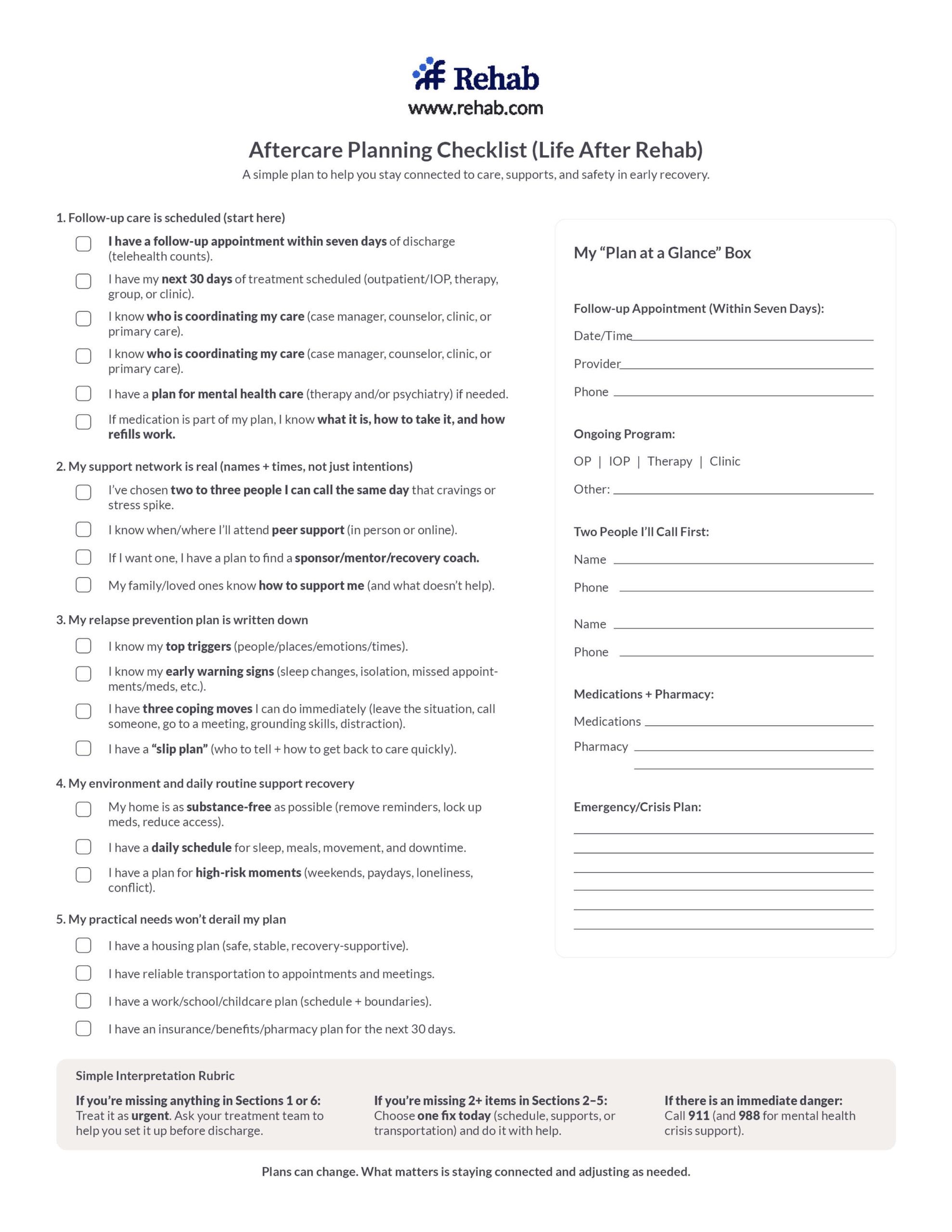
Aftercare
Drug rehab aftercare refers to the ongoing support structure a person maintains after completing a formal treatment program. It typically combines a step-down level of care, continued therapy, a support group, and in many cases continued medication. The period immediately following discharge from treatment is the highest-risk window for relapse, making aftercare planning one of the most consequential elements of the full treatment experience.

How to choose the right level of care
The right starting level of care depends on four factors working together: the severity of the substance use disorder (mild, moderate, or severe as defined by DSM-5 diagnostic criteria), the substance or substances involved, the presence of co-occurring medical or mental health conditions, and the stability of the person’s home environment and social support.
People with severe SUD, significant withdrawal risk from alcohol or benzodiazepines, active suicidal ideation, or an unstable living situation need a medically supervised setting as a starting point. People with milder presentations, strong social support, and no major medical complications may do well beginning in intensive outpatient care.
The ASAM patient placement criteria exist specifically to guide this matching process. A clinical assessment using these criteria, which most treatment programs offer at no cost during intake, is the gold standard for determining appropriate care. People commonly both underestimate and overestimate the intensity they need, and a trained clinician is better positioned to make that call than the person trying to evaluate themselves in the middle of a crisis.
One practical note: if outpatient treatment has been tried before and did not hold, a higher level of care is usually indicated. Prior treatment history is one of the most reliable predictors of appropriate placement.
Online and telehealth addiction treatment
Virtual addiction treatment, including online intensive outpatient programs and telehealth counseling, expanded substantially after 2020 and is now an established care option.6 It is appropriate for people with mild-to-moderate SUD who have a stable, private home environment, reliable internet access, and no significant medical withdrawal risk. Many programs offer a hybrid model that combines virtual sessions with periodic in-person visits.
Virtual treatment is not appropriate as the sole treatment option for people with severe physical dependence, high overdose risk, or unstable housing. For those individuals, a residential or medically supervised setting is the safer starting point.
Medication-assisted treatment (MAT)
Medication-assisted treatment uses FDA-approved medications alongside behavioral therapy to treat opioid use disorder and alcohol use disorder. SAMHSA and NIDA identify MAT as the gold standard of care for opioid use disorder, with strong evidence that it reduces illicit opioid use, lowers overdose risk, and helps people stay in treatment longer.7
Opiates
For opioid use disorder, the primary FDA-approved medications are:
- Methadone: a long-acting opioid agonist that reduces cravings and withdrawal without producing a significant high at therapeutic doses. Dispensed through licensed opioid treatment programs.
- Buprenorphine (Suboxone): a partial opioid agonist that reduces cravings and withdrawal. Prescribable by licensed clinicians in office-based settings.
- Naltrexone (Vivitrol): an opioid antagonist that blocks the euphoric effect of opioids. Requires full detox before starting.
Alcohol
For alcohol use disorder, FDA-approved medications include:
- Naltrexone: reduces cravings for alcohol and the rewarding effect of drinking.
- Acamprosate: helps reduce post-acute withdrawal symptoms including anxiety and sleep disruption.
- Disulfiram (Antabuse): causes an unpleasant physical reaction if alcohol is consumed, creating a deterrent to drinking.
A common concern about MAT is that it amounts to replacing one addiction with another. This reflects a misunderstanding of how these medications work. At therapeutic doses, medications like buprenorphine and methadone stabilize brain chemistry and reduce compulsive drug-seeking without producing the euphoria that drives addictive behavior. They are medical treatments for a medical condition, and withholding them on the basis of this misconception has measurable consequences for patient outcomes.7
MAT is most effective when combined with counseling and social support. Medication alone is not a complete treatment.

Therapy and behavioral treatment
Behavioral therapy is a core component of virtually every addiction treatment program, at every level of care. The primary goal is to identify the thoughts, emotions, and situations that drive substance use and build concrete skills to manage them differently. The most widely used evidence-based approaches are:
Cognitive behavioral therapy
Cognitive behavioral therapy (CBT) teaches people to recognize distorted or unhelpful thinking patterns that contribute to substance use, and to replace them with more accurate and productive responses. It is highly adaptable and has a strong evidence base across addiction and co-occurring mental health conditions.
Dialectical behavior therapy
Dialectical behavior therapy (DBT) was originally developed for borderline personality disorder and is now widely used in addiction treatment, particularly for people with difficulty regulating emotions or who have a history of self-harm. Its core skills modules cover mindfulness, distress tolerance, emotional regulation, and interpersonal effectiveness.
Motivational interviewing
Motivational interviewing (MI) is a client-centered counseling approach that helps people explore ambivalence about change and build internal motivation to engage with treatment. It is frequently used in early treatment stages and with people who are not yet fully committed to recovery.
12-step Facilitation
12-step group therapy helps people engage with Alcoholics Anonymous, Narcotics Anonymous, or similar peer-support programs as part of their recovery. Research supports 12-step participation as a useful complement to clinical treatment, particularly for long-term sobriety maintenance.8
Group therapy
Group therapy provides a structured context for peers in recovery to share experiences, give and receive feedback, and practice interpersonal skills. It is a standard component of both inpatient and outpatient programs and offers benefits that individual therapy alone cannot.
Individual therapy and group therapy are not interchangeable; most comprehensive programs use both. The specific combination of modalities in a person’s treatment plan should be tailored to their presenting issues, substance use history, and co-occurring conditions.

Treating co-occurring mental health conditions
Two out of three people who enter addiction treatment have at least one co-occurring mental health condition.9 Depression, anxiety, PTSD, bipolar disorder, and ADHD are the most common. The relationship between addiction and mental health runs in both directions: mental health conditions increase the risk of substance use disorder, and sustained heavy use can trigger or worsen psychiatric symptoms.
Treating only the substance use disorder while leaving a mental health condition unaddressed significantly increases the likelihood of relapse. The clinical standard for people with co-occurring conditions is integrated treatment that addresses both simultaneously, with licensed mental health clinicians as part of the treatment team.
When evaluating a program, ask directly whether they have licensed mental health clinicians on staff, whether psychiatric assessment is part of the intake process, and whether they can prescribe psychiatric medications independently of the addiction treatment plan. Programs that silo mental health care from addiction care are generally less effective for people with complex presentations.
See our dual diagnosis guide for detail on specific co-occurring conditions including depression, anxiety, PTSD, bipolar disorder, and ADHD.

Specialty treatment programs
Some programs are designed for specific populations. For many people, finding a program that reflects their particular circumstances improves engagement and, in turn, outcomes. Specialty programs available in the U.S. include:
- Veterans: Programs addressing the specific intersection of military service, combat trauma, and PTSD with substance use. VA and community-based options are available.
- Adolescents and teens: Programs with age-appropriate treatment, family involvement, and school coordination.
- Women: Programs addressing trauma, domestic violence history, childcare, and gender-specific health considerations.
- LGBTQ+ individuals: Affirming programs that address discrimination-related trauma and community-specific risk factors.
- Working professionals and executives: Programs with flexible scheduling, confidentiality protections, and executive-focused programming.
- Families with children: Residential programs that allow mothers and children to remain together during treatment.
- Faith-based programs: Programs that integrate spiritual practices and community as part of the recovery framework.
- Holistic programs: Programs that incorporate yoga, mindfulness, acupuncture, and nutrition alongside clinical care.

Support groups and peer recovery
Peer support is one of the most consistent predictors of long-term recovery, and it is largely accessible at no cost. Addiction support groups are not a substitute for clinical treatment, but they are a meaningful complement, particularly in the months and years after formal treatment ends.
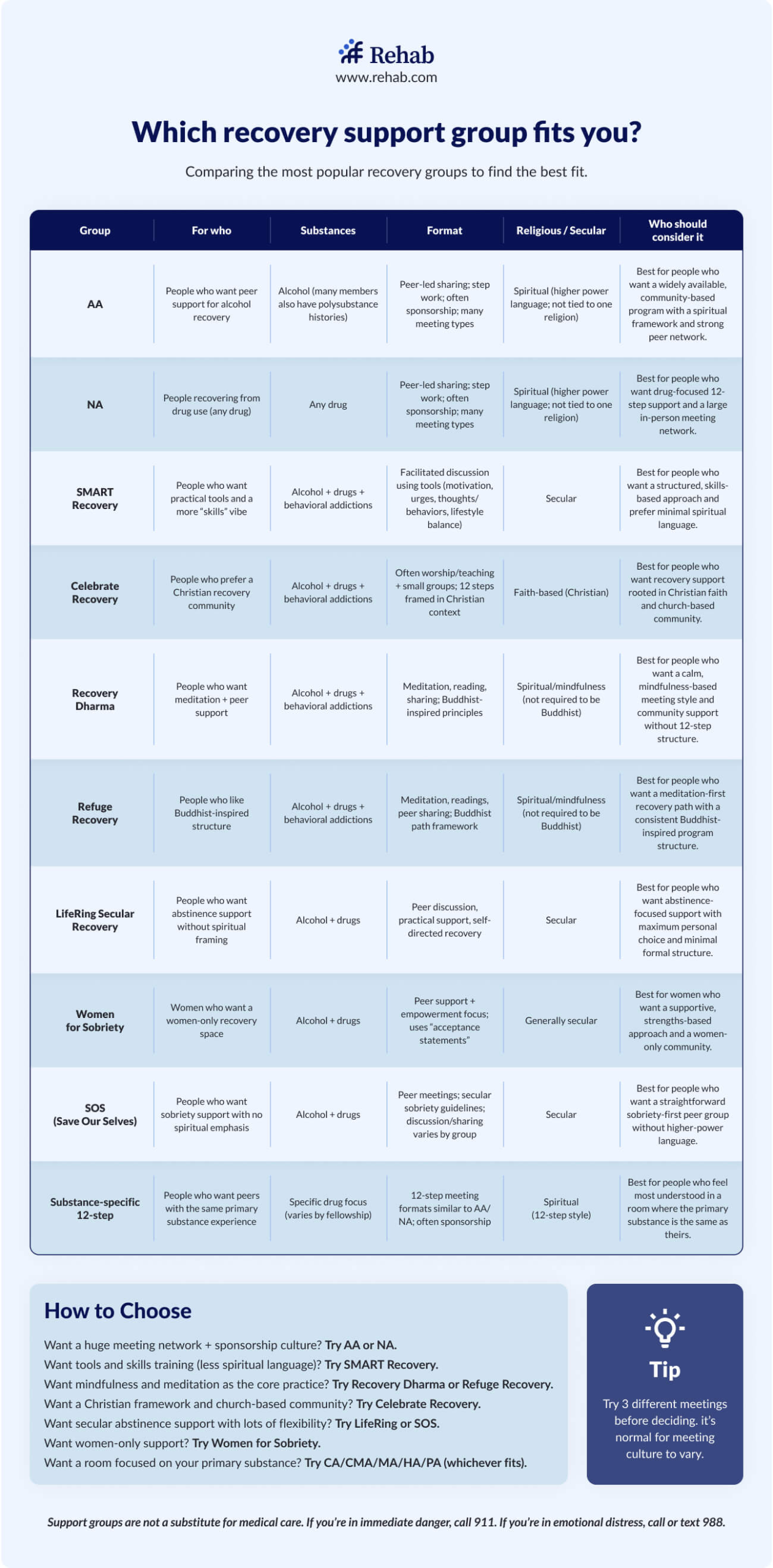
The two most widely available options are:
12-step
Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) use a 12-step model built around acceptance, community accountability, and working through a structured set of principles. Both have global meeting networks and are free to attend. Research has found that regular attendance is associated with improved long-term abstinence rates.8
Non 12-step
SMART Recovery takes a secular, evidence-based approach focused on self-management and behavioral skills. It does not use the 12-step model or spiritual language. Meetings are available in-person and online. It is a well-regarded option for people who do not connect with the AA/NA framework.
Many people use support groups alongside ongoing therapy and MAT rather than as a standalone approach. Different models work for different people, and trying more than one is common.

How much does addiction treatment cost?
Treatment costs vary widely depending on level of care, program length, and location. As a general range, outpatient programs may cost a few hundred to a few thousand dollars per month, while standard inpatient residential programs typically run between $6,000 and $20,000 for a 30-day stay.

Most people do not pay the full cost out of pocket. Coverage mechanisms that commonly apply include:
- Private insurance under the ACA: Under the Affordable Care Act, substance use disorder treatment is classified as an essential health benefit, and most major insurance plans are required to cover it at parity with medical and surgical benefits. The Mental Health Parity and Addiction Equity Act (MHPAEA) prohibits insurers from imposing more restrictive coverage limits on SUD treatment than on other medical conditions.10
- Medicaid: Medicaid covers a broad range of addiction treatment services in all states, including detox, inpatient, outpatient, and MAT. Eligibility and specific covered services vary by state.
- Medicare: Medicare Part A covers inpatient treatment, Part B covers outpatient services, and Part D covers prescription medications including MAT.
- State-funded programs: Every state operates publicly funded substance use treatment programs for people without insurance or with low income. Availability and wait times vary.
- Sliding-scale fees: Many non-profit and community-based treatment programs adjust fees based on income and ability to pay.
See our detailed guides to how much rehab costs, how to pay for rehab, and free and low-cost rehab options.
What to look for in a treatment center
When choosing a program, there are five concrete quality markers worth confirming:
State licensure and accreditation
A quality treatment program will be licensed by the state in which it operates and accredited by a recognized third-party body. The most well-known accreditation organizations are the Commission on Accreditation of Rehabilitation Facilities (CARF) and The Joint Commission. Accreditation requires a rigorous facility evaluation and signals that the program meets defined standards of care. SAMHSA maintains a public treatment locator that includes licensed programs.
Evidence-based clinical approaches
Ask specifically whether the program uses CBT, DBT, motivational interviewing, and/or 12-step facilitation therapy. Programs that cannot name their clinical modalities or rely primarily on non-evidence-based approaches warrant scrutiny. Holistic and experiential therapies are valuable adjuncts, but they should complement clinical treatment, not replace it.
Staff credentials
Ask whether the clinical team includes licensed addiction counselors, licensed mental health clinicians, and, for programs offering MAT, prescribing physicians or advanced practice providers. Programs with high staff-to-patient ratios and appropriate credentialing provide more individualized care.
Dual diagnosis capacity
Given that the majority of people in treatment have a co-occurring mental health condition, confirm that the program can assess and treat mental health conditions alongside the SUD, rather than referring out.
Aftercare planning
Ask at intake what the discharge planning process looks like. Programs that send people home without a concrete aftercare plan are leaving the highest-risk period unaddressed. A clear step-down plan, including ongoing therapy, support group connection, and continued MAT where applicable, is a basic quality indicator.
Rehab.com’s Rehab Score and Transparency Report explains how facilities are evaluated and ranked on this site, including the specific data points used to assess quality.
What happens after treatment?
The period immediately after formal treatment ends is the most vulnerable window for relapse. Comprehensive aftercare planning closes the gap between the structure of a program and the demands of ordinary life.

Effective aftercare typically combines several elements at once:
- A step-down to a lower level of care, moving from inpatient to IOP or from IOP to standard outpatient, maintains clinical support while restoring daily independence.
- Continued individual or group therapy addresses the ongoing psychological work that does not end at discharge.
- A support group provides peer accountability and community.
- Sober living may provide a transitional housing option for people who are not ready to return to their previous home environment.
- And continued MAT, where applicable, maintains the neurological stabilization that reduces relapse risk.
Relapse is common in recovery from addiction, as it is in other chronic conditions. When it occurs, it does not signal that treatment has failed. It signals a need to re-engage treatment, potentially at a higher level of care, and to review what was missing from the aftercare plan.
Treatment FAQs
Look for state licensure, accreditation by CARF or The Joint Commission, named evidence-based clinical modalities, appropriate staff credentials, dual diagnosis capacity, and a clear aftercare planning process. Rehab.com’s Rehab Score methodology explains how programs are evaluated. A trained admissions advisor can also help match your clinical needs to an appropriate program at no cost.
A clinical assessment using ASAM patient placement criteria is the most reliable way to determine the appropriate starting level. Most treatment programs offer this assessment at no cost during intake. As a general guide, severe SUD, significant withdrawal risk, or an unstable home environment typically indicate a need for medically supervised residential care. Mild-to-moderate SUD with a stable support system may be appropriately addressed in intensive outpatient care.
Inpatient rehab is residential: the person lives at the treatment facility and receives care 24 hours a day. Outpatient rehab allows the person to live at home and attend treatment sessions for a set number of hours per week. Inpatient is more intensive and appropriate for severe SUD or unstable home environments. Outpatient is more flexible and appropriate for milder presentations or as a step-down after inpatient care.
Program lengths range from seven to ten days for medical detox through 30-, 60-, or 90-day inpatient programs to ongoing outpatient treatment lasting several months. NIDA research consistently finds that treatment lasting 90 days or more is associated with better outcomes than shorter programs.2 Recovery is a long-term process; formal treatment is the structured beginning of it, not the entirety.
Most major insurance plans are required under the Affordable Care Act to cover substance use disorder treatment as an essential health benefit, and the Mental Health Parity and Addiction Equity Act prohibits insurers from imposing more restrictive limits on SUD treatment than on other medical conditions.10 Medicaid and Medicare also cover a range of treatment services. The specific covered services and cost-sharing vary by plan; verification of benefits before admission is strongly recommended.
No. At therapeutic doses, medications like methadone and buprenorphine stabilize brain chemistry and reduce compulsive drug-seeking behavior without producing the euphoria that drives addiction. They are medical treatments for a medical condition. SAMHSA, NIDA, and ASAM all identify MAT as evidence-based care and recommend against withholding it based on this misconception.7
It depends on the level of care. Intensive outpatient programs are specifically designed to accommodate work schedules, typically holding sessions in the morning or evening. Standard outpatient allows even more flexibility. Inpatient and PHP programs require a more substantial daily time commitment that is generally incompatible with full-time work during treatment.
Find Addiction Treatment Centers
Finding facilities near you…
References
- Substance Abuse and Mental Health Services Administration. 2023 National Survey on Drug Use and Health (NSDUH): Results. Rockville, MD: SAMHSA; 2024.
- National Institute on Drug Abuse. Principles of drug addiction treatment: A research-based guide, Third Edition. Updated January 2018. https://nida.nih.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition. Accessed March 2026.
- American Society of Addiction Medicine. The ASAM criteria: Treatment criteria for addictive, substance-related, and co-occurring conditions. Rockville, MD: ASAM; 2013.
- Substance Abuse and Mental Health Services Administration. Detoxification and substance abuse treatment: Treatment Improvement Protocol (TIP) Series, No. 45. Rockville, MD: SAMHSA; 2015.
- Polcin DL, Korcha R, Bond J, Galloway G. Sober living houses for alcohol and drug dependence: 18-month outcomes. J Subst Abuse Treat. 2010;38(4):356-365. doi:10.1016/j.jsat.2010.02.003. See also: National Alliance for Recovery Residences. 2020 National Recovery Housing Survey. Cited in Mericle AA, et al. J Subst Abuse Treat. 2021;120:108153.
- Hser Y-I, Mooney LJ, Balyan M, et al. Telehealth and in-person delivery of intensive outpatient buprenorphine treatment during COVID-19. J Subst Abuse Treat. 2022;140:108791.
- Substance Abuse and Mental Health Services Administration. Medications for opioid use disorder: Treatment Improvement Protocol (TIP) Series 63. Rockville, MD: SAMHSA; 2021.
- Kelly JF, Humphreys K, Ferri M. Alcoholics Anonymous and other 12-step programs for alcohol use disorder. Cochrane Database Syst Rev. 2020;3(3):CD012880. doi:10.1002/14651858.CD012880.pub2.
- Substance Abuse and Mental Health Services Administration. Co-occurring disorders and other health conditions. Updated 2023. https://www.samhsa.gov/co-occurring-disorders. Accessed March 2026.
- U.S. Department of Labor. The Mental Health Parity and Addiction Equity Act. https://www.dol.gov/agencies/ebsa/laws-and-regulations/laws/mental-health-parity. Accessed March 2026.





