
































































































Inpatient drug and alcohol rehab provides 24/7, live-in treatment that helps you safely navigate detox, stabilize, and start rebuilding your life in a highly structured environment. In this guide, you’ll learn who inpatient care is best for, how long it lasts, what it costs, and how to choose the best inpatient drug rehab centers to support lasting recovery.
Key Points
- Inpatient rehab is residential treatment that provides 24/7 medical and clinical care for moderate to severe substance use disorders.
- Programs typically run 30, 60, or 90 days, with long-term options available for chronic addiction or complex co-occurring conditions.
- Most inpatient programs begin with medical detox, then move into individual therapy, group therapy, family work, and aftercare planning.
- The Affordable Care Act requires most private insurance, Medicaid, and Medicare plans to cover substance use disorder treatment as an essential health benefit.
- Inpatient costs vary widely, ranging from roughly $5,000 to $30,000 for a 30-day stay, with luxury or specialty programs costing more.
- Strong programs are state-licensed, accredited by CARF or The Joint Commission, and use evidence-based therapies for addiction and mental health.
In This Article:
- What is inpatient drug rehab?
- Who should consider inpatient rehab?
- What happens during inpatient treatment?
- Therapies used in inpatient rehab
- How long does inpatient rehab last?
- How much does inpatient rehab cost?
- Does insurance cover inpatient rehab?
- Inpatient vs outpatient rehab
- What to look for in an inpatient rehab center
- What happens after inpatient rehab?
- Inpatient rehab FAQs
What Is Inpatient Drug Rehab?
Inpatient drug rehab, also called residential treatment, is a live-in program where a person stays at a treatment center for the duration of care while receiving 24-hour medical supervision, daily structured therapy, and a substance-free environment. It is the most intensive non-hospital level of addiction care and is typically used for people with moderate to severe substance use disorders or significant co-occurring conditions.1
| Level of care | Who is this for | Average daily cost | Medical supervision | Length of stay | Time required |
|---|---|---|---|---|---|
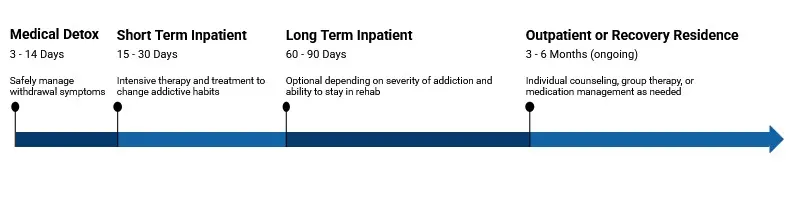
| Medical detox | Severe withdrawal, high-risk cases | $500 to $1,000 | 24/7 medical staff | 3 to 14 days | Full-day monitoring |
| Inpatient | Co-occurring disorders, chronic use | $300 to $800 | 24/7 clinical support | 30 to 90 days | Full-day, live-in |
| Intensive outpatient | Employed, stable home, relapse risk | $100 to $300 | Limited, non-medical | 8 to 12 weeks | 3 to 5 hours/day, 3 to 5 days/week |
| Outpatient | Mild use, early-stage recovery | $50 to $150 | Minimal or none | Varies, often ongoing | 1 to 2 hours/week or as needed |
The American Society of Addiction Medicine (ASAM) Criteria, which most U.S. clinicians and insurers use to place people in the right level of care, classifies residential and inpatient care as Level 3 and Level 4 services. Level 3 programs are clinically managed residential services at varying intensity, and Level 4 is medically managed intensive inpatient care for people who need around-the-clock physician supervision.2
Inpatient programs differ from medical detox, which focuses narrowly on managing withdrawal, and from outpatient programs, which allow a person to live at home while attending treatment sessions. Most inpatient stays include or are preceded by detox, then transition into a longer therapeutic phase that addresses the psychological, behavioral, and social drivers of substance use.
Who Should Consider Inpatient Rehab?
Inpatient rehab is generally appropriate for people with moderate to severe substance use disorders, those at risk of dangerous withdrawal, and anyone whose home environment makes outpatient recovery unsafe or impractical. A clinical assessment, usually guided by the ASAM Criteria, helps match a person to the right level of care based on six dimensions, including withdrawal risk, medical and psychiatric stability, motivation, relapse history, and living environment.2
The National Institute on Drug Abuse (NIDA) notes that no single treatment is right for everyone. Effective care is tailored to a person’s medical, mental health, and substance use history, as well as their family situation, work or school context, and any co-occurring conditions.3 Inpatient care is most often recommended when at least one of the following applies:
- Severe physical dependence on alcohol, benzodiazepines, opioids, or stimulants, where withdrawal could be medically dangerous without supervision.
- Co-occurring mental health conditions such as depression, anxiety, PTSD, or bipolar disorder that need integrated treatment alongside addiction care.
- Prior treatment that did not hold, including multiple outpatient attempts or relapses after detox.
- An unstable or high-risk home environment, such as living with active substance use, exposure to violence, or housing instability.
- Significant medical needs related to addiction, such as liver disease, heart complications, or pregnancy with substance use.
- A need for structure in early recovery, especially for people who have struggled to maintain abstinence on their own.
For people with chronic substance use disorders and a history of repeated relapse, residential care of 90 days or longer is often associated with stronger long-term outcomes than shorter stays.3 A treatment provider or primary care physician can complete an ASAM assessment and recommend the right level of care.
What Happens During Inpatient Treatment?
Inpatient treatment usually follows four phases: admission and assessment, medical detox and stabilization, active treatment with structured therapy, and aftercare planning. Most days follow a planned schedule of individual therapy, group sessions, education, peer support, and structured downtime, all delivered in a substance-free residential setting with around-the-clock staff.1
Admission typically begins with a clinical and medical intake to identify substances used, withdrawal risk, co-occurring conditions, medications, and treatment goals. Bloodwork, urine screening, and a psychiatric assessment are common. The care team then builds an individualized treatment plan with measurable goals and assigns a primary therapist or case manager.
1. Admission & Assessment
A clinical intake, insurance verification, medical and psychiatric evaluation, and individualized treatment plan with measurable recovery goals.
Medically supervised withdrawal management lasting roughly 3 to 10 days, with comfort medications and 24/7 nursing care to keep the body safe.
3. Active Treatment
A structured daily mix of individual therapy, group sessions, family work, education, and peer support to address the drivers of substance use.
A discharge plan with continued outpatient therapy, support groups, medication management, and sober-living options to protect early recovery.
A typical inpatient day blocks out time for breakfast, morning group, individual therapy or a clinical appointment, a midday process group, an afternoon skills or psychoeducation session, an evening 12-step or peer-support meeting, and personal time. Meals, sleep, and movement are part of the clinical model, since nutrition and rest support brain recovery during early sobriety.
Family involvement is encouraged at most accredited programs. Family therapy sessions, education days, and visitation help repair relationships and prepare loved ones to support the person after discharge.
Therapies Used in Inpatient Rehab
Most inpatient programs build treatment around evidence-based behavioral therapies, with medication-assisted treatment (MAT) added when clinically appropriate. NIDA identifies behavioral therapies, including cognitive behavioral therapy and contingency management, as the most commonly used forms of substance use disorder treatment, often combined with FDA-approved medications for opioid and alcohol use disorders.3

A strong inpatient program will combine several of the following modalities into a personalized weekly schedule:
- Cognitive behavioral therapy (CBT): Identifies the thoughts, feelings, and triggers that drive substance use and teaches new coping skills to manage cravings and high-risk situations.
- Dialectical behavior therapy (DBT): Combines CBT skills with mindfulness, distress tolerance, and emotion regulation. Often used for clients with co-occurring borderline personality disorder, self-harm history, or chronic suicidality.
- Motivational interviewing (MI): A collaborative, client-centered approach that helps strengthen a person’s own motivation and commitment to change.
- Group therapy: Daily process and skills groups facilitated by a clinician, which reduce isolation and let participants learn from peers further along in recovery.
- Individual therapy: One-on-one sessions with a primary therapist that work through trauma, family dynamics, grief, and other underlying issues.
- Family therapy: Sessions that address communication, boundaries, codependency, and the impact of addiction on the family system.
- Medication-assisted treatment (MAT): FDA-approved medications such as buprenorphine, methadone, naltrexone, and acamprosate, used to reduce cravings and prevent relapse for opioid or alcohol use disorders.
- Relapse-prevention planning: A structured curriculum to identify personal triggers, warning signs, and step-by-step responses to high-risk moments.
- Holistic and experiential therapies: Yoga, meditation, art therapy, equine therapy, exercise, and nutrition counseling are common add-ons that support overall well-being but should not replace evidence-based care.
Programs that treat people with both addiction and mental health conditions should offer integrated dual diagnosis care, where psychiatric medications, therapy for the mental health condition, and addiction treatment are delivered by one coordinated team. SAMHSA recommends this integrated model over treating the conditions in sequence or in separate programs.4
Call A Treatment Provider
For a conversation about what treatment options are available to you.
Make a Call
How Long Does Inpatient Rehab Last?
Most inpatient programs run 30, 60, or 90 days, with long-term residential programs lasting 6 to 12 months for chronic addiction or complex co-occurring conditions. NIDA notes that research has consistently shown that participation of 90 days or longer is associated with better outcomes, including reduced relapse rates and improved long-term recovery.3
Insurance authorization, the severity of the substance use disorder, withdrawal complexity, and the presence of co-occurring conditions all influence how long an individual stays. The clinical team usually reassesses progress every 7 to 14 days and adjusts the level of care accordingly.
- 30-day programs: The most common length, often the default starting point. Suited for early or moderate substance use disorders and people with strong outside support.
- 60-day programs: Allow more time for behavioral change, family work, and relapse-prevention skill building. A common choice for people stepping down from a complicated detox or with a prior relapse.
- 90-day programs: Often recommended for people with chronic addiction, multiple relapses, or co-occurring mental health diagnoses. Associated with stronger long-term outcomes than shorter stays.
- Long-term rehab (6 to 12+ months): Therapeutic-community models, sober living, and modified residential programs that focus on whole-life rebuilding for the most severe cases.

How Much Does Inpatient Rehab Cost?
Inpatient rehab costs vary widely based on the program length, the level of medical care, the geographic location, and the amenities offered. A standard 30-day inpatient program in the United States typically runs between roughly $5,000 and $30,000 out of pocket. Luxury or executive programs can cost $40,000 to $80,000 or more for the same length of stay.
The figures below are out-of-pocket cost estimates for self-pay clients before insurance, financing, or sliding-scale adjustments. Most people do not pay the sticker price because insurance covers most or all of the cost.
| Level of care | Typical cost range | Duration |
|---|---|---|
| Medical detox | $500 to $1,000 per day | 3 to 10 days |
| Inpatient / residential rehab | $300 to $800 per day | 30, 60, or 90 days |
| Long-term residential | $300 to $800 per day | 6 to 12+ months |
| Partial hospitalization program (PHP) | $250 to $600 per day | 2 to 4 weeks typical |
| Intensive outpatient program (IOP) | $200 to $500 per day | 8 to 12 weeks typical |
| Standard outpatient | $50 to $250 per day | Often 3 to 6 months |
Several factors influence the final price: facility location, private versus shared rooms, medical staffing ratio, the inclusion of medical detox in the same admission, ancillary services such as psychiatric care or specialty programming, and contracted insurance rates. State-funded and nonprofit programs offer sliding-scale fees and free care for qualifying individuals.

Does Insurance Cover Inpatient Rehab?
In most cases, yes. The Affordable Care Act classifies mental health and substance use disorder services as one of the ten essential health benefits, which means most marketplace, employer-sponsored, Medicaid, and Medicare plans are required to provide some coverage for addiction treatment, including inpatient rehab.5 Coverage levels, in-network requirements, prior authorization rules, and length-of-stay limits vary by plan.

Federal mental health parity law also requires that insurer rules for mental health and substance use treatment, including copays, deductibles, and visit limits, be no more restrictive than rules for medical or surgical care.5 In practice, this means a plan generally cannot make it harder to get covered inpatient addiction care than it would for a comparable medical hospitalization.
- Private insurance: Most major carriers, including Blue Cross Blue Shield, Aetna, Cigna, UnitedHealthcare, and Humana, cover inpatient rehab when the treatment is medically necessary and the facility is in-network.
- Medicaid: Covers substance use disorder treatment in all 50 states, with the scope and provider network varying by state. Many state Medicaid programs cover inpatient detox and residential treatment.
- Medicare: Covers medically necessary inpatient SUD treatment under Part A and outpatient services under Part B. Coverage criteria mirror standard hospital-based care.
- TRICARE and VA benefits: Cover inpatient SUD treatment for active-duty service members, retirees, and eligible veterans, including community-care referrals when VA capacity is limited.
- Self-pay, financing, and sliding scale: Many programs offer payment plans, health-care lending partners, or income-based sliding-scale rates. State-funded programs may provide free care for qualifying individuals.
Before admission, call the facility’s admissions team or your insurer’s behavioral health number to verify benefits, confirm the in-network status, and check whether prior authorization is required. Ask for a written estimate of out-of-pocket costs and the criteria the plan uses to authorize continued stay.

Inpatient vs Outpatient Rehab
The main difference between inpatient and outpatient rehab is whether a person lives at the facility. Inpatient rehab requires a residential stay with 24/7 supervision, while outpatient rehab allows a person to live at home and attend treatment on a scheduled basis. Both formats use the same evidence-based therapies. The right choice depends on addiction severity, medical and psychiatric stability, home environment, and personal responsibilities.1
| Feature | Inpatient rehab | Outpatient rehab |
|---|---|---|
| Living arrangement | Lives at the treatment facility for the duration of care | Lives at home, attends scheduled sessions |
| Supervision | 24/7 staff supervision and medical access | Limited to session hours |
| Typical hours of care per week | Full immersion; daily clinical programming | 3 to 20+ hours per week, depending on level (PHP, IOP, OP) |
| Best fit for | Moderate to severe SUD, withdrawal risk, co-occurring disorders, unstable home | Mild to moderate SUD, stable home, work or school obligations, step-down care |
| Typical duration | 30, 60, or 90 days; long-term programs 6 to 12 months | 8 weeks to 6+ months, varies by program |
| Cost (self-pay) | $5,000 to $30,000+ for 30 days | $1,400 to $10,000 for 30 days; IOP programs $3,000 to $10,000 |
| Insurance coverage | Covered when medically necessary; prior authorization usually required | Covered; usually fewer authorization barriers |
Many people move through the continuum of care rather than choosing one or the other. A common path is medical detox, then inpatient rehab, then a partial hospitalization program (PHP), then an intensive outpatient program (IOP), then standard outpatient and aftercare support. This step-down model lets a person taper supervision as recovery skills strengthen.
What to Look for in an Inpatient Rehab Center
A quality inpatient program will be state-licensed, accredited by a recognized body, staffed by credentialed clinicians, and built around evidence-based therapies and aftercare planning. Marketing claims, scenic photos, and amenities are not substitutes for clinical quality, so the evaluation should focus on credentials, treatment approach, and outcomes.
- State licensure: Every legitimate inpatient program holds a current license from its state’s behavioral health or health-services agency.
- Independent accreditation: Look for accreditation from CARF (the Commission on Accreditation of Rehabilitation Facilities), The Joint Commission, or LegitScript. Accreditation signals that the program meets independent standards for safety, ethics, and clinical quality.
- Evidence-based therapies: The program should clearly describe its use of CBT, DBT, motivational interviewing, family therapy, and medication-assisted treatment when clinically appropriate.
- Credentialed staff: Licensed clinicians (LCSW, LMFT, LPC, LCDC, RN, MD, psychiatrist) and a clear medical director. Staff-to-client ratios are a useful proxy for attention and safety.
- Dual diagnosis capability: If a co-occurring mental health condition is present, the program should offer integrated dual diagnosis treatment, including psychiatric medication management.
- Individualized treatment planning: A formal assessment, written treatment plan with measurable goals, and regular plan reviews.
- Family involvement: Structured family programming, family therapy sessions, and clear visitation and communication policies.
- Strong aftercare planning: A written discharge plan with appointments scheduled before leaving, peer-support introductions, and clear medication continuity.
- Transparent pricing and insurance: A clear pre-admission financial estimate, written insurance verification, and direct contact with billing staff.
Be cautious of programs that promise guaranteed outcomes, advertise unusually aggressive marketing or 24/7 cold calls, refuse to share licensure or accreditation details, charge for travel arrangements that resemble patient brokering, or pressure for an immediate admission. The Federal Trade Commission has warned about deceptive marketing in the addiction treatment industry, and SAMHSA recommends verifying licensure with the state agency directly.
Call A Treatment Provider
For a conversation about what treatment options are available to you.
Make a Call
What Happens After Inpatient Rehab?
Inpatient rehab is the start of recovery, not the finish line. A strong discharge plan steps a person down through progressively less intensive care, including outpatient therapy, medication management when relevant, peer support, and stable housing. NIDA describes substance use disorder as a chronic, treatable condition that often requires ongoing management to sustain recovery, similar to other chronic illnesses.3
Typical aftercare components include:
- Step-down clinical care: A PHP, IOP, or standard outpatient program to continue therapy while resuming work, school, or family responsibilities.
- Sober living homes: Structured drug-free residences that bridge the gap between inpatient care and full independent living.
- Continued MAT: Ongoing buprenorphine, methadone, naltrexone, or acamprosate when clinically indicated, with regular prescriber follow-up.
- Peer support and mutual aid: 12-step groups, SMART Recovery, Refuge Recovery, and other community-based programs that provide accountability and connection.
- Mental health follow-up: Continued psychiatric care, therapy for trauma or mood disorders, and consistent medication management.
- Lifestyle and wellness habits: Sleep, nutrition, movement, social connection, and meaningful daily structure that support long-term sobriety.
Relapse is part of the picture for many people. NIDA reports that relapse rates for substance use disorders are comparable to those for other chronic illnesses such as type 1 diabetes, hypertension, and asthma, ranging from roughly 40% to 60%.3 A return to use does not mean treatment failed. It signals the need to re-engage care, often at a higher level.

Inpatient Drug Rehab FAQs
What is the difference between inpatient and residential rehab?
The terms are often used interchangeably. Strictly speaking, ASAM uses “inpatient” (Level 4) to describe medically managed care in a hospital-like setting and “residential” (Level 3) to describe clinically managed live-in care of varying intensity. In everyday use, both refer to live-in addiction treatment programs.2
Can I bring my phone, laptop, or work materials?
Policies vary widely. Many programs restrict phone and internet use during the first phase of treatment to reduce outside distractions, then allow scheduled access later. Executive and professional programs often offer more lenient policies. Confirm the rules in writing during admissions.
Can someone be admitted involuntarily?
In limited circumstances, yes. About half of U.S. states have civil commitment laws that allow a court to order substance use treatment for a person who poses a risk to themselves or others. Most inpatient admissions, however, are voluntary, often preceded by a formal intervention.
What about work and the FMLA?
Eligible employees of covered employers can use the Family and Medical Leave Act (FMLA) for up to 12 weeks of unpaid, job-protected leave for treatment of a serious health condition, which includes substance use disorder treatment that requires inpatient care or continuing treatment by a health care provider.6 Many employers also offer paid medical leave or short-term disability benefits.
Will my employer or family find out?
Federal regulations (42 CFR Part 2) protect the confidentiality of substance use treatment records. Treatment providers cannot share records without written consent except in narrow legal circumstances. HIPAA also applies to general medical records. A person can usually attend inpatient rehab without their employer being notified of the specific reason for medical leave.
What if I cannot afford inpatient rehab?
Options include Medicaid coverage, state-funded programs, nonprofit and faith-based providers, sliding-scale fees, scholarship beds at some facilities, payment plans, and health-care lending. SAMHSA’s National Helpline (1-800-662-HELP) is free and confidential and can connect a person to state-funded treatment. See how to get insurance to pay for rehab treatment.
Find Inpatient Rehab Centers
Finding facilities near you…
Finding facilities near you…
Finding facilities near you…
References
- Substance Abuse and Mental Health Services Administration. Treatments for Substance Use Disorders. SAMHSA. https://www.samhsa.gov/substance-use/treatment. Accessed June 1, 2026.
- Mee-Lee D, ed. The ASAM Criteria: Treatment Criteria for Addictive, Substance-Related, and Co-Occurring Conditions. 4th ed. American Society of Addiction Medicine; 2023.
- National Institute on Drug Abuse. Drugs, Brains, and Behavior: The Science of Addiction. Treatment and Recovery. NIDA. Updated 2025. https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/treatment-recovery. Accessed June 1, 2026.
- Substance Abuse and Mental Health Services Administration. Substance Use Disorder Treatment for People With Co-Occurring Disorders: Treatment Improvement Protocol (TIP) Series, No. 42. SAMHSA Publication No. PEP20-02-01-004. 2020. https://library.samhsa.gov/product/tip-42-substance-use-treatment-persons-co-occurring-disorders/pep20-02-01-004. Accessed June 1, 2026.
- Centers for Medicare & Medicaid Services. Mental Health and Substance Use Disorder Parity. CMS. https://www.cms.gov/marketplace/private-health-insurance/mental-health-parity-addiction-equity. Accessed June 1, 2026.
- U.S. Department of Labor, Wage and Hour Division. Fact Sheet #28: The Family and Medical Leave Act. https://www.dol.gov/agencies/whd/fact-sheets/28-fmla. Accessed June 1, 2026.
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2023 National Survey on Drug Use and Health. HHS Publication No. PEP24-07-021. 2024. https://www.samhsa.gov/data/report/2023-nsduh-annual-national-report. Accessed June 1, 2026.
- Substance Abuse and Mental Health Services Administration. Co-Occurring Disorders and Other Health Conditions. SAMHSA. Updated 2026. https://www.samhsa.gov/substance-use/treatment/co-occurring-disorders. Accessed June 1, 2026.





