
































































































Alcohol withdrawal side effects are common when the body adjusts to the absence of alcohol after prolonged use. Headaches are one such side effect of alcohol withdrawal that often accompanies alcohol withdrawal.
This article examines the causes of headaches during withdrawal, their typical duration and strategies for managing them. You’ll also learn about other related symptoms, potential risks and treatment options.
Whether you’re preparing for detox or supporting someone going through it, this guide provides practical insights to help navigate the withdrawal process safely and effectively.
Key Facts
- Headaches are a frequent symptom of alcohol withdrawal due to chemical changes in the brain.
- Symptoms usually begin within 6 to 24 hours after the last drink and may peak within 2 to 3 days.
- Dehydration, disrupted sleep and nervous system overactivity can worsen headaches.
- Managing withdrawal safely may require medical supervision in some cases.
- Treatment options include hydration, medications and structured detox programs.
- Untreated withdrawal can lead to serious complications such as seizures or delirium tremens.
In This Article
- What Are Alcohol Withdrawal Headaches?
- Hangover vs. Withdrawal vs. Migraine
- Why It Happens & Who’s at Risk
- Home Relief vs. Medical Care
- When to Seek Urgent Care
- Preventing Future Episodes
- FAQs
- Find Treatment
What Are Alcohol Withdrawal Headaches?
Alcohol withdrawal headaches are a common early symptom of alcohol withdrawal syndrome (AWS), typically starting 6 to 24 hours after the last drink and peaking between 24 and 72 hours.
They result from neurochemical rebalancing as the brain adjusts to the absence of alcohol and are often accompanied by anxiety, tremors, and elevated blood pressure. Most withdrawal headaches resolve within several days, but severe or worsening symptoms should prompt medical evaluation.
Healthcare providers often use tools like the Clinical Institute Alcohol Withdrawal Assessment for Alcohol Scale to assess symptom severity1 and guide safe and personalized care.
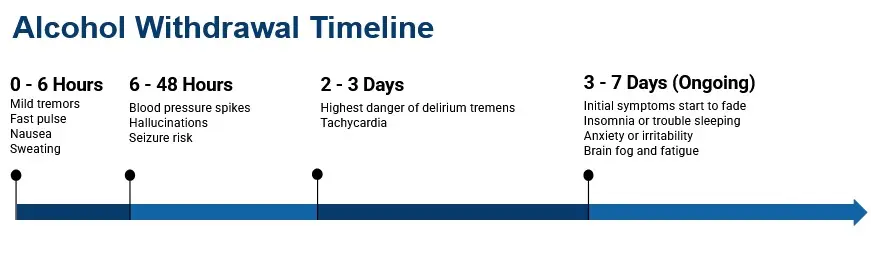
When It Starts, Peaks and Resolves
Understanding the alcohol withdrawal timeline can help you anticipate when headaches are likely to appear and how long they may last.
Headaches from alcohol withdrawal usually begin within 6 to 24 hours after the last drink. They often peak in intensity between 24 and 72 hours3,4, and gradually improve as the nervous system stabilizes and the body adjusts to the absence of alcohol.
Alcohol withdrawal headaches often cluster with other symptoms such as rapid heart rate, elevated blood pressure, nausea, sweating, irritability and insomnia. While these symptoms are typically temporary it’s essential to closely monitor any changes.
If headaches become severe, progressively worsen or persist beyond several days, professional medical evaluation is recommended.
In some cases untreated withdrawal can escalate to serious complications such as seizures or delirium tremens. This makes early intervention crucial for safety and recovery.
Hangover vs. Withdrawal vs. Migraine: How to Tell
A hangover headache follows a single drinking episode and resolves within 24 hours. An alcohol withdrawal headache appears 6 to 24 hours after reducing or stopping heavy, prolonged drinking and can persist for several days alongside symptoms like tremors and anxiety. A migraine can occur anytime and typically causes one-sided, pulsating pain with light and sound sensitivity.
Distinguishing between these three types is important because withdrawal headaches may signal a condition that requires medical attention.
Key Differences
Hangover headaches typically occur within hours of drinking and resolve within 24 hours. These types of headaches usually involve dehydration, fatigue and stomach upset that will normally improve with rest and hydration.
Withdrawal headaches develop 6 to 24 hours after reducing or stopping heavy drinking and can last several days3. They may also involve tremors, anxiety, sweating, nausea and sleep disturbances.
Migraine headaches can occur anytime and may be unrelated to alcohol. They’re often triggered by stress, hormones or specific foods. These types of headaches frequently cause pulsating, one-sided pain, sensitivity to light and sound and sometimes a visual aura.
Why It Matters
Mislabeling alcohol withdrawal as a “hangover” can delay necessary medical care. If headaches are severe, persistent, or paired with worsening symptoms, it’s safest to seek professional evaluation to rule out withdrawal complications or other urgent conditions.
Why It Happens & Who’s at Risk
Alcohol withdrawal headaches are caused by neurochemical rebound, specifically a drop in GABA activity and a surge in glutamate, that produces central nervous system hyperexcitability after chronic alcohol exposure ends. Dehydration, electrolyte imbalances, and disrupted sleep can worsen symptoms.
People with a history of heavy daily drinking, prior withdrawal seizures, older age, concurrent medical conditions, or polysubstance use face higher risk and should seek supervised care rather than managing withdrawal at home.
Neurochemical Rebound + Common Contributors
Alcohol withdrawal headaches occur due to neurochemical rebound after chronic alcohol exposure. When drinking stops abruptly, the brain experiences a GABA downshift and glutamate surge, leading to central nervous system (CNS) hyperexcitability and headache3,5.
Other factors can worsen headache severity during withdrawal, including dehydration, electrolyte imbalances, skipped meals, poor sleep and sudden caffeine changes.
Individuals with pre-existing headache disorders or a history of migraines often experience amplified withdrawal related pain5.
Higher Risk Situations (When Home Care Isn’t Appropriate)
Certain situations require medical supervision rather than at home management. These include:
- Heavy daily drinking or history of withdrawal seizures or delirium tremens (DTs)1
- Older age, pregnancy, or significant medical/psychiatric conditions
- Polysubstance use involving sedatives, opioids, or other depressants
- Limited social support or unstable housing
In these cases, supervised detox and closer monitoring are safer and reduce the risk of serious complications, including seizures and severe withdrawal syndromes.
Professional care ensures proper hydration, medication management and symptom control during recovery.
Alcohol Withdrawal Headache Treatment: Home Relief vs. Medical Care
Mild alcohol withdrawal headaches can often be managed with hydration, electrolyte replacement, small frequent meals, and rest in a low-stimulation environment. Over-the-counter pain relievers should be used cautiously due to liver and gastrointestinal risks associated with heavy drinking.
Moderate to severe withdrawal typically requires clinical treatment with benzodiazepines guided by CIWA-Ar scoring, along with thiamine supplementation and supportive IV care. The appropriate treatment setting (outpatient or inpatient) depends on symptom severity and patient risk factors.
Safe self-care (and OTC cautions)
For mild alcohol withdrawal headaches, self care strategies may ease discomfort. Focus on hydration with electrolytes, small, frequent meals to stabilize blood sugar and rest in a dark, quiet space to reduce sensory overload.
Relaxation techniques may also provide relief. Try deep breathing, guided imagery or gentle stretching to help ease your symptoms, Applying a cool compress to the forehead may help reduce headache intensity.
Over the counter medications should be used with caution. The pain reliever, acetaminophen, should be used sparingly due to liver stress in heavy drinkers.
NSAIDs such as ibuprofen and naproxen can increase the risk of developing or worsening gastrointestinal bleeding and should be avoided if an individual has ulcers or bleeding disorders.
Never combine over the counter medications with alcohol or sedatives unless recommended by your doctor. Limit combination or quick release analgesics to reduce rebound headaches.
Avoid “relief drinking” because repeated withdrawal episodes from stopping and restarting alcohol use can worsen withdrawal severity; This is known as the kindling effect.
How Clinicians Treat AWS (and When Outpatient vs. Inpatient)
Clinicians assess the severity of withdrawal symptoms using tools like the CIWA-Ar scale to guide treatment and management.
Benzodiazepinesare the first line pharmaceutical therapy for moderate to severe alcohol withdrawal1,2 by reducing CNS hyperexcitability and helping to prevent seizures. Thiamine or vitamin B1 is given early to protect against Wernicke-Korsakoff syndrome1.
Additionally, supportive care often includes IV fluids, electrolyte correction and antiemetics for nausea. In some mild cases gabapentin or carbamazepine may be used as adjunctive treatment1.

Determining the appropriate level of care depends on a patient’s risk level as determined by their CIWA-Ar scores. Outpatient care is appropriate for low risk, stable patients with reliable social support.
Inpatient detox or ICU care is recommended for those with high CIWA-Ar scores, a history of seizures or delirium tremens, significant medical or psychiatric comorbidities or unstable living situations.
Proper treatment planning ensures safety, symptom control and a smoother recovery process.
Call A Treatment Provider
For a conversation about what treatment options are available to you.
Make a Call
When to Seek Urgent Care for Alcohol Withdrawal
Seek emergency medical care immediately if you experience seizures, hallucinations, severe confusion, high fever, chest pain, a sudden severe headache, uncontrolled vomiting, or rapidly rising blood pressure during alcohol withdrawal. These symptoms may indicate life-threatening complications such as delirium tremens or cardiac events. Supervised medical care is the safest way to manage severe alcohol withdrawal.
Red Flags You Shouldn’t Ignore
Certain alcohol withdrawal symptoms require immediate medical attention.
Seek emergency care if you experience:
- Seizures, hallucinations, severe confusion or delirium
- A high fever, chest pain, or a sudden “thunderclap” or worst ever headache
- Uncontrolled vomiting, severe dehydration or fainting
- Rapidly rising blood pressure or heart rate
If any of these red flags are present, or if symptoms worsen after 72 hours, call emergency services or go to the nearest ER immediately. Prompt evaluation can prevent serious complications, including delirium tremens, cardiac events and life threatening electrolyte imbalances.
Never attempt to manage severe alcohol withdrawal alone. Supervised care ensures safety and effective treatment.
When Headaches Persist: Post-Acute Withdrawal Syndrome (PAWS)
Most alcohol withdrawal headaches resolve within the first week after a person’s last drink. For some people, however, headaches and other symptoms can return or linger for weeks to months as part of a condition known as post-acute withdrawal syndrome (PAWS).
PAWS occurs because the brain continues to recalibrate its neurochemistry long after acute withdrawal ends. During this period, a person may experience recurring headaches alongside mood swings, difficulty concentrating, sleep disturbances, and heightened sensitivity to stress. These symptoms tend to come and go in waves rather than remaining constant, and they generally decrease in frequency and intensity over time.
Several factors increase the likelihood of experiencing prolonged withdrawal symptoms, including a longer history of heavy alcohol use, prior withdrawal episodes (which may intensify symptoms through the kindling effect), and co-occurring mental health conditions such as anxiety or depression.
Managing PAWS-related headaches involves many of the same strategies used during acute withdrawal — maintaining consistent hydration, regular sleep schedules, balanced nutrition, and stress management. Working with a healthcare provider can help identify whether ongoing headaches are related to PAWS or to another medical condition that needs separate attention.
Ongoing participation in a structured outpatient treatment program or recovery support group can provide accountability and reduce the isolation that often accompanies protracted recovery symptoms.
Preventing Future Episodes
The most effective strategy for preventing alcohol withdrawal headaches is treating the underlying alcohol use disorder. FDA-approved medications, behavioral therapies like CBT, and peer support groups can reduce cravings and sustain recovery. Planning medically supervised withdrawal for future quit attempts lowers the risk of severe symptoms, including headaches that may worsen with repeated withdrawal episodes.
The best way to prevent alcohol withdrawal headaches is to treat the underlying alcohol use disorder (AUD). Evidence based options include medications like naltrexone, acamprosate or disulfiram6,7 in select cases.
These should be combined with counseling such as cognitive behavioral therapy (CBT) or motivational enhancement therapy (MET) and peer support groups.
For future quit attempts, plan a medically supervised withdrawal and create a release-prevention toolkit focusing on healthy sleep, balanced meals, stress management and trigger awareness.
Utilize treatment locators and helplines to find local detox programs and ongoing care.
FAQs
They are often worse in the first 72 hours after the last drink and usually improve within several days. Any persistent or worsening symptoms that last beyond a week should be evaluated by a medical professional.
Hangover headaches follow a single drinking episode and resolve in less than 24 hours.
Withdrawal headaches last longer and may include other symptoms, including anxiety, insomnia, tremors or elevated vital signs and should be evaluated by medical professionals.
Use only under medical advice, as both carry risks with heavy alcohol use.
Individuals experiencing seizures, hallucinations, confusion, high fever, chest pain, sudden severe headache, severe nausea and vomiting or signs of dehydration should go to the ER immediately.
On their own, withdrawal headaches are uncomfortable but not life-threatening. They become a safety concern when they appear alongside more severe withdrawal symptoms such as seizures, hallucinations, confusion, or dangerously elevated blood pressure. A sudden, extremely severe headache (aka “thunderclap” headache) during withdrawal also warrants emergency evaluation. If headaches worsen rather than improve over the first few days, or if they are accompanied by any of the red-flag symptoms listed above, seek medical attention promptly.
Sleep is often disrupted during withdrawal, and headaches can make it harder to rest. Keeping the room dark, cool, and quiet may help. A consistent bedtime routine, avoiding screens before sleep, and gentle relaxation techniques such as deep breathing or progressive muscle relaxation can support sleep quality. Caffeine should be limited, especially in the afternoon and evening. If insomnia persists and significantly interferes with recovery, a healthcare provider can evaluate whether short-term medication support is appropriate.
They can. Some people experience recurring headaches weeks or even months after their last drink as part of post-acute withdrawal syndrome (PAWS). These episodes tend to be less intense than acute withdrawal headaches and typically become less frequent over time. Maintaining consistent hydration, regular sleep, balanced nutrition, and ongoing recovery support helps reduce the likelihood and severity of recurring symptoms.
Find Alcohol Withdrawal Management Near You
Use our rehab center locator to find the best treatment centers based on location, level of care, insurance coverage, and special programs.
Call
800-985-8516
( ![]() Sponsored Helpline )
to speak with someone for personalized assistance.
Sponsored Helpline )
to speak with someone for personalized assistance.
Resources
- American Society of Addiction Medicine (ASAM). The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management. J Addict Med. 2020;14(3S):1-72. https://www.asam.org/quality-care/clinical-guidelines/alcohol-withdrawal-management-guideline
- National Institute on Alcohol Abuse and Alcoholism (NIAAA). Alcohol Use Disorder: From Risk to Diagnosis to Recovery. NIAAA Core Resource on Alcohol. Updated 2025. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/alcohol-use-disorder-risk-diagnosis-recovery
- Alcohol Withdrawal Syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; Updated February 2024. https://www.ncbi.nlm.nih.gov/books/NBK441882/
- MedlinePlus. Alcohol Withdrawal. U.S. National Library of Medicine. https://medlineplus.gov/ency/article/000764.htm
- Son H, Zhang Y, Shannonhouse J, Ishida H, Gomez R, Kim YS. Mast-cell-specific receptor mediates alcohol-withdrawal-associated headache in male mice. Neuron. 2023;111(24):4019-4035.e7. doi:10.1016/j.neuron.2023.09.039
- Substance Abuse and Mental Health Services Administration (SAMHSA). Medication for the Treatment of Alcohol Use Disorder: A Brief Guide. HHS Publication No. SMA15-4907. https://store.samhsa.gov/product/medication-treatment-alcohol-use-disorder-brief-guide/sma15-4907
- National Institute on Alcohol Abuse and Alcoholism (NIAAA). Understanding Alcohol Use Disorder. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/understanding-alcohol-use-disorder





