
































































































Alcohol withdrawal medications are essential for safely managing symptoms, preventing complications and supporting recovery after stopping heavy or prolonged drinking.
When you reduce or discontinue alcohol use, your body experiences significant changes in brain chemistry that can lead to uncomfortable and sometimes dangerous withdrawal symptoms.
This guide provides a clear overview of how clinicians assess withdrawal severity, choose appropriate medications and determine the safest treatment setting based on your risk factors.
Key Facts
- Alcohol withdrawal medications are critical for safely managing symptoms, preventing complications and supporting recovery after stopping heavy or prolonged drinking.
- Withdrawal can produce mild to life threatening symptoms, with urgent care required if you experience confusion, seizures, hallucinations, fever or unstable vital signs.
- Symptoms often follow a timeline: 6–24 hours (early signs), 24–48 hours (seizure risk) and 48–96 hours (highest risk for delirium tremens).
- Clinicians use tools like CIWA-Ar and PAWSS, along with ASAM criteria, to determine if you require inpatient vs. outpatient care and appropriate medication strategies.
- Benzodiazepines remain the first line treatment, with delivery methods such as symptom triggered dosing, fixed tapers or front loading tailored to patient needs.
- Adjunct medications (clonidine, gabapentin, phenobarbital, thiamine) may support recovery, while naltrexone after detox reduces cravings and relapse risk.
What is Alcohol Withdrawal?
Alcohol withdrawal is a set of physical and neurological symptoms that occur when a person with heavy or prolonged alcohol use suddenly reduces or stops drinking. Symptoms can range from mild tremors and anxiety to life-threatening seizures and delirium tremens, making medical supervision essential for safe recovery.
Alcohol withdrawal occurs when your body and central nervous system react to the sudden absence of alcohol after heavy or prolonged use. This process can cause a range of symptoms that vary in intensity, making proper understanding and medical support essential for safety and recovery.

What It Is, Who’s at Risk and When to Seek Urgent Care
Your body becomes accustomed to alcohol’s depressant effects and reacts with hyperexcitability during withdrawal, leading to symptoms that can range from mild to life threatening. People with the highest risk have a history of severe withdrawal, prior seizures or delirium tremens (DTs).
People with a high alcohol tolerance, older adults and those with significant medical conditions are also more vulnerable. Early recognition and proper medical supervision are essential to manage symptoms safely and prevent serious complications during alcohol withdrawal.
Symptoms that indicate you require urgent or emergency attention include confusion, hallucinations, seizures, fever, unstable blood pressure or heart rate and persistent severe vomiting.
Symptom Timeline
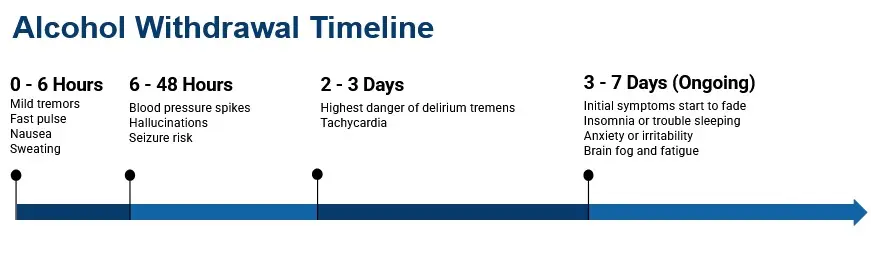
Alcohol withdrawal can be life threatening without medical supervision. Early recognition of alcohol withdrawal symptoms and proper treatment are critical to preventing complications and ensure safe recovery.
Here’s a rough breakdown of what to expect in the initial hours of alcohol withdrawal:
- 6-24 hours: Early signs like tremors, anxiety, sweating and insomnia often appear.
- 24-48 hours: Symptoms intensify with worsening heart rate, blood pressure and possible seizures.
- 48-96 hours: Highest risk for DTs, marked disorientation, worsening heart rate, blood pressure and possible seizures.
Why Repeated Withdrawal Episodes Increase Risk
Each time a person goes through alcohol withdrawal without adequate medical management, the brain can become more sensitive to future withdrawal episodes. This phenomenon, known as kindling, means that symptoms may become more severe with each subsequent withdrawal, even if the person’s recent drinking was less intense than in the past.
Kindling is one of the key reasons clinicians recommend medically supervised detox rather than repeated attempts to stop drinking without support. People with a history of multiple withdrawal episodes are at higher risk for seizures and delirium tremens, and their treatment plans may require more aggressive medication protocols from the start.
Assessment & Care Setting: How Clinicians Decide and What to Expect
Clinicians determine your level of care by evaluating symptom severity, medical history, and psychosocial stability using evidence-based tools like the CIWA-Ar scale and ASAM placement criteria. This assessment decides whether you receive treatment in an inpatient or outpatient setting and which medication strategy is safest for your situation.
Inpatient vs. Outpatient Care
Inpatient treatment is recommended for more severe cases and higher withdrawal risks, when one or more of the following applies:
- A history of severe withdrawal, seizures or DTs
- Unstable housing
- Polysubstance use (particularly sedatives)
- Significant medical or psychiatric comorbidities
- Unreliable follow up or long-term support
Outpatient care may be appropriate when you have mild to moderate symptoms, stable home support and access to daily medical monitoring.
Clinical Assessment Tools
There are two commonly used alcohol withdrawal assessments that physicians use to determine your withdrawal risk:
- PAWSS (Prediction of Alcohol Withdrawal Severity Scale): Screens patients before withdrawal begins to identify when you have high risk factors for complications, ensuring safer care placement and better outcomes.
- CIWA-Ar (Clinical Institute Withdrawal Assessment for Alcohol): Measures withdrawal severity and informs symptom triggered medication dosing. Higher scores typically indicate that the level of inpatient care and monitoring should be escalated.
The CIWA-Ar scale rates 10 symptoms on a point system, producing a total score between 0 and 67. Clinicians typically interpret scores as follows:
- Below 10 (Mild): Supportive care; medication may not be needed
- 10 to 18 (Moderate): Consider medication; reassess frequently
- 19 and above (Severe): Active pharmacologic treatment indicated; escalate monitoring
Higher scores signal greater risk for complications such as seizures or delirium tremens, and they help clinicians decide when to move from outpatient observation to inpatient care.

First Line Alcohol Withdrawal Medications: Benzodiazepines
Benzodiazepines are the gold standard treatment for managing alcohol withdrawal syndrome (AWS), because they effectively control agitation, tremors, seizures and the risk of delirium tremors (DTs). Clinicians select a specific benzodiazepine and dosing strategy based on symptom severity, liver function, age, and care setting.
By calming overactive brain activity, these medications help stabilize you during withdrawal. Clinicians carefully select the appropriate medication, dosage and treatment strategy based on symptom severity, co occurring conditions, medical history and care setting to ensure safety and improve recovery outcomes.
How Treatment Is Delivered

Alcohol withdrawal treatment can be delivered in several ways, with the approach tailored to symptom severity and care setting. Methods vary from symptom based dosing to scheduled tapers, front loading strategies and different routes of administration to ensure safety and effective recovery.
- Symptom Triggered Dosing: Preferred when close monitoring is possible. Medication is given only when symptoms emerge based on CIWA-Ar scores, reducing total drug exposure and recovery time.
- Fixed Tapers: Scheduled doses gradually decrease over several days. This is used when frequent monitoring isn’t feasible, such as in outpatient settings.
- Front Loading: High initial doses for long acting benzodiazepines rapidly stabilize severe withdrawal and prevent complications in high risk patients.
- Routes of Administration: Oral (PO) is preferred for stable patients, while IV or IM dosing is reserved for severe agitation, vomiting or poor absorption.
Benzodiazepine selection depends on withdrawal severity, comorbidities and monitoring capacity. Choosing the right agent and dosing strategy improves safely, reduces complications, and supports a smoother recovery.
Diazepam (Valium)
Diazepam is a fast-acting, long-lasting medication frequently used in high-dose protocols to rapidly stabilize severe alcohol withdrawal and prevent seizures. However, its prolonged effects require careful monitoring and reduced dosing for older adults or individuals with impaired liver function.
Advantages
Rapid onset and long half life make diazepam ideal for front loading protocols and seizure prevention
Disdvantages
Use lower doses in liver-impaired and older adults to avoid oversedation or respiratory depression.
Chlordiazepoxide (Librium)
Widely recognized as a staple for outpatient alcohol withdrawal tapers, Chlordiazepoxide offers a smooth, long-acting reduction in withdrawal symptoms. Because it is heavily processed by the liver, clinicians must carefully adjust dosages for patients with a history of hepatic dysfunction.
Advantages
A long acting option commonly used in outpatient tapers. It provides smoother withdrawal with fewer breakthrough symptoms.
Disdvantages
Heavily metabolized by the liver. Dose adjustments are needed for liver dysfunction. You must avoid alcohol and be warned about operating machinery.
Lorazepam (Ativan)
Lorazepam is a versatile, intermediate-acting option that is highly effective for symptom-triggered treatment, especially when nausea requires IV or intramuscular administration. It is often the safest frontline choice for older adults and individuals with liver disease because it bypasses the heavy hepatic processing required by other medications.
Advantages
Intermediate half life and reliable IM/IV absorption make it useful for symptom triggered protocols and when you have nausea or vomiting.
Disdvantages
Preferred in older adults and those with liver disease since it bypasses extensive hepatic metabolism.
Clonazepam (Klonopin)
While less commonly studied as a frontline medication for alcohol withdrawal syndrome, Clonazepam can serve as an effective supplementary treatment to manage lingering anxiety and tremors. Clinicians typically reserve it for specialized cases or as an adjunct therapy, monitoring patients closely to prevent oversedation.
Advantages
Can help reduce anxiety and tremor when other benzodiazepines are contraindicated or are insufficient.
Disdvantages
Less studied as a first line AWS treatment. It’s generally used as an adjunct or when standard agents are contraindicated. Monitor closely for cumulative sedation.
| Medication | Primary Use in Alcohol Care | Typical Course | Common Side Effects |
|---|---|---|---|
| Librium (chlordiazepoxide) | First-line treatment for moderate-to-severe withdrawal; prevents seizures and delirium tremens | 3 to 7 days, tapered | Drowsiness, dizziness, coordination issues |
| Gabapentin | Mild-to-moderate withdrawal; reduces anxiety and cravings | 5 to 7 days, tapered | Dizziness, fatigue, swelling |
| Clonidine | Adjunct medication for high blood pressure, sweating, and anxiety; does not prevent seizures | 3 to 5 days | Low blood pressure, dry mouth, drowsiness |
| Naltrexone (oral or Vivitrol injection) | Post-detox craving and reward reduction | Daily oral or monthly injection; often long-term | Nausea, headache, fatigue |
| Thiamine (Vitamin B1) | Prevents Wernicke-Korsakoff syndrome; routinely given during alcohol detox | Daily during detox, often parenteral | Generally well tolerated |
For reference only. Medication decisions belong with a licensed clinician.
Adjuncts & Alternative Withdrawal Medications
Adjunctive medications can help manage alcohol withdrawal symptoms but are not substitutes for benzodiazepines, which remain the first line treatment. These drugs are used selectively to target specific symptoms, reduce overall medication needs and manage complications when appropriate.
In certain cases, they also improve your comfort, support stabilization and address co-occurring mental health conditions or underlying medical issues during the withdrawal process. Adjunctive therapies should be customized to your needs and used only under medical supervision to optimize safety and outcomes.
Clonidine
Clonidine helps ease autonomic symptoms such as rapid heart rate, hypertension and sweating. It is used only as an adjunct therapy in your alcohol withdrawal and not independently, since it does not prevent seizures or DTs. Your blood pressure should be monitored closely because of the risk of hypertension.
Gabapentin
Gabapentin may be considered if you have mild alcohol withdrawal symptoms or to manage sleep disturbance and anxiety during your early recovery. In some cases, it can reduce benzodiazepine requirements.
However, there is a potential for misuse, and it can cause addictive sedation, especially when combined with alcohol or other depressants. Your renal function should be assessed before treatment.
Phenobarbital
Phenobarbital, a barbiturate, is reserved for severe or benzodiazepine refractory withdrawal, often in ED or ICU settings under close supervision. It has a narrow therapeutic window and increases the risk of respiratory depression. Using phenobarbital requires continuous monitoring by experienced clinicians.
Thiamine (Vitamin B1)
Thiamine is essential for preventing Wernicke’s encephalopathy(a neurological emergency caused by lack of thiamine [vitamin B1]), especially if you have malnutrition, liver disease or homelessness.
It must be administered before glucose and given parenterally in moderate-to-severe withdrawal or if you have poor nutritional status. After IV administration, it can be followed by oral maintenance therapy.
Carbamazepine (Tegretol)
Carbamazepine is an anticonvulsant that may be used for mild alcohol withdrawal when benzodiazepines are not indicated or when a clinician wants to minimize sedation. Some guidelines, including recommendations from Cleveland Clinic and the AAFP, list carbamazepine as a first-line option for patients whose withdrawal is mild and not expected to progress.
It can help reduce anxiety, tremors, and the risk of seizure recurrence. It also carries a lower potential for misuse compared to benzodiazepines. However, carbamazepine does not prevent delirium tremens and is not appropriate as a standalone treatment for moderate to severe withdrawal. Side effects can include dizziness, nausea, and rare but serious blood count changes, so monitoring is recommended during treatment.
Beta-Blockers
Beta-blockers such as atenolol or propranolol may be used as adjuncts to manage persistent elevated heart rate and high blood pressure during alcohol withdrawal. They can also help reduce tremors and anxiety symptoms.
Beta-blockers do not prevent seizures or delirium tremens and should never be used as standalone treatment for alcohol withdrawal. They are most appropriate when autonomic symptoms persist despite adequate benzodiazepine dosing. Your clinician will monitor your heart rate and blood pressure closely if a beta-blocker is added to your care plan.
THC (Cannabis)
Although this is commonly used to self medicate for sleep or anxiety THC is not recommended during withdrawal. Evidence is insufficient and it may worsen cognition, anxiety and may have interactions with sedatives. Safer recovery focused alternatives should be discussed instead.
Nearby Alcohol Rehabs
Finding facilities near you…
After Alcohol Withdrawal: Medications for Alcohol Use Disorder
After the withdrawal phase, certain medications can support your long term recovery by reducing cravings and the risk of relapse. Naltrexone is one of the most prescribed options, helping to block the rewarding effects of alcohol and promote sustained sobriety.

Naltrexone for Alcohol Withdrawal
Naltrexone is a first line option for relapse prevention after completing alcohol withdrawal.
It works by reducing your cravings and lowering the risk of heavy drinking days. Treatment should begin only after acute withdrawal resolves and opioid free status is confirmed to avoid precipitated withdrawal.
Two forms are available:
- Oral naltrexone (daily dosing) offers flexibility and is easier to discontinue if side effects occur.
- Extended release (XR) naltrexone is given monthly by injection to improve adherence in patients struggling with daily compliance.
Before starting therapy, clinicians should check your liver enzymes, discuss opioid blockage effects and provide education on integrating naltrexone with counseling, peer support and behavioral therapies for best outcomes.

Acamprosate (Campral) for Alcohol Withdrawal
Acamprosate helps restore the balance between excitatory and inhibitory brain signaling that chronic alcohol use disrupts. It is prescribed after withdrawal is complete and works best for people who have already stopped drinking and want to maintain sobriety.
Unlike naltrexone, acamprosate does not block the effects of alcohol or opioids. It is generally well tolerated, with diarrhea as the most common side effect. Because it is eliminated through the kidneys rather than the liver, acamprosate may be a better choice for people with liver disease who need long-term medication support.

Disulfiram (Antabuse) for Alcohol Withdrawal
Disulfiram works through aversion: it blocks the enzyme that breaks down alcohol in the body, causing unpleasant physical reactions (flushing, nausea, rapid heartbeat) if a person drinks while taking it.
Disulfiram does not reduce cravings and requires strong personal motivation and adherence, since a person can simply stop taking the medication before drinking. It is most effective as part of a supervised treatment program where adherence can be monitored. Disulfiram is not appropriate for people with severe liver disease, heart conditions, or those who may be exposed to alcohol unknowingly.

Safety, Interactions & Special Populations
Alcohol withdrawal medications can interact with other substances and carry additional risks for certain populations, including older adults, people with liver disease, and those who are pregnant. Clinicians must review your full medication list and medical history before prescribing to reduce the chance of dangerous drug interactions.
Personalized treatment plans and continuous monitoring improve safety, reduce complications and ensure better outcomes during withdrawal management, especially for these vulnerable populations.
High Risk Drug Combinations
Avoid combining benzodiazepines with alcohol, opioids or other sedatives, as they can cause severe respiratory depression, coma or death. You and your clinician should review medication lists and substance use before prescribing.
Clinicians typically start with lower doses and titrate slowly in older adults because of an increased sensitivity to drugs and the risk of falls. Lorazepam is preferred if you have liver impairment since it relies less on liver metabolism.
Pregnancy, Postpartum & Co Occurring Substance Use
If you are pregnant or postpartum your care should be managed in higher acuity settings with OB collaboration for fetal monitoring and breastfeeding safety.
When there’s co use of opioids, stimulants or other sedatives, clinicians should integrate overdose prevention strategies, provide naloxone education and coordinate comprehensive treatment plans for your and your infant’s safety.
FAQs About Alcohol Withdrawal
Home detox is not recommended when you have moderate to severe alcohol withdrawal symptoms or a high risk history (e.g. seizures, DTs, unstable vitals or liver disease).
Complications can be life threatening without supervision. If detoxing at home, safety improves with a clinical assessment, daily monitoring, home support and a clear escalation plan in case symptoms worsen.
Chlordiazepoxide (Librium) and diazepam (Valium) are long acting benzodiazepines.
Diazepam acts faster, making it ideal for front loading protocols, while Librium is commonly used in outpatient tapers. When you have liver disease, lorazepam may be a safer alternative.
No, gabapentin may help with mild withdrawal, anxiety and sleep disturbances, but it’s not reliable for a seizure or DTs prevention. It should only be used under a clinician’s supervision and monitor for sedation or misuse risk.
Giving glucose first can trigger Wernicke’s encephalopathy (a neurological emergency caused by lack of thiamine [vitamin B1]) in thiamine deficient patients. Thiamine protects the brain and is given before glucose, often by IV in high-risk patients.
Not recommended. THC may worsen anxiety, paranoia and sedation risks when combined with other medications. Safer, non sedative sleep strategies should be discussed with a clinician.
Lorazepam is typically preferred for AWS in patients with liver problems, while long acting benzodiazepines should be used cautiously. Coordinate care with hepatology and monitor closely for over sedation.
Find Treatment for Alcohol Withdrawal
Finding the right treatment center for alcohol withdrawal and recovery can feel overwhelming, but help is available.
Use a trusted directory where you can search and compare treatment centers based on your specific needs. You can filter options by location, level of care, insurance coverage and special programs to find a facility that matches your situation.
If you’re unsure where to begin, support is just a phone call away. Call
800-985-8516
( ![]() Sponsored Helpline )
today to speak with someone who can explain your treatment options, answer your questions and guide you toward safe, effective care.
Sponsored Helpline )
today to speak with someone who can explain your treatment options, answer your questions and guide you toward safe, effective care.
Starting treatment is an important step toward recovery. Whether you need detox, inpatient rehab, outpatient care or specialized programs, having the right resources makes the process easier and more personalized to your needs.
References
- Choudhary M, Braria A, Sharma V, Mathur A. Alcohol Withdrawal Syndrome: Benzodiazepines and Beyond. J Clin Diagn Res. 2015;9(9):VE01-VE07.
- American Society of Addiction Medicine. The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management. J Addict Med. 2020;14(3S):1-72.
- Substance Abuse and Mental Health Services Administration. 2024 National Survey on Drug Use and Health: Detailed Tables. SAMHSA; 2025.
- National Institute on Alcohol Abuse and Alcoholism. Alcohol Facts and Statistics. NIAAA; 2025.
- Jesse S, Brathen G, Ferrara M, et al. Alcohol withdrawal syndrome: mechanisms, manifestations, and management. Acta Neurol Scand. 2017;135(1):4-16.
- World Health Organization. Management of Alcohol Withdrawal. mhGAP Evidence Centre. WHO; 2023.
- Mirijello A, D’Angelo C, Ferrulli A, et al. Identification and management of alcohol withdrawal syndrome. Drugs. 2015;75(4):353-365.




