
































































































Sedatives are central nervous system depressants prescribed for anxiety, insomnia, and seizures. When used outside a prescription, tolerance can build quickly and lead to dependence, addiction, and dangerous withdrawal. This guide walks through how sedatives work, how to recognize a problem, and what addiction treatment options look like.
Key Points
- Sedatives are central nervous system depressants prescribed for anxiety, insomnia, and seizures, and most are controlled substances under federal law.
- The main sedative classes are benzodiazepines, barbiturates, non-benzodiazepine sleep aids (Z-drugs), and the veterinary tranquilizers like xylazine.
- Sedative withdrawal can be medically dangerous and may include seizures, which is why detox usually requires a supervised taper rather than abrupt cessation.
- Sedative use disorder is diagnosed using DSM-5-TR criteria and is treated with a combination of medical detox, behavioral therapy, and ongoing recovery support.
- Combining sedatives with opioids, alcohol, or other depressants greatly raises the risk of fatal overdose.
In This Article
- Understanding Sedative Addiction
- Common Types of Sedative Drugs
- Signs and Symptoms of Sedative Abuse
- The Dangers and Risks of Sedative Addiction
- Sedative Withdrawal and Detoxification
- Sedative Addiction Treatment
- Frequently Asked Questions
- Find Treatment Near You
Understanding Sedative Addiction
Sedatives are medications that are typically prescribed for anxiety, sleep issues or seizures. These central nervous system (CNS) depressants slow brain activity, helping users feel calm and relaxed, and they are safe when used as directed. However, when misused, a person can develop dependence and be at a high risk of addiction.
4.6 million Americans aged 12 or older misused prescription tranquilizers or sedatives in the past year, according to the most recent National Survey on Drug Use and Health.1
What Drugs Are Sedatives?
Sedatives are a broad class of drugs that act as CNS depressants, slowing brain activity to produce calming effects. However, tolerance can develop quickly with many sedatives, meaning that the body needs higher doses over time to achieve the same results.
This rapid tolerance can contribute to a cycle of misuse, as individuals may take increasing amounts to maintain the desired effects, ultimately raising the risk of dependence and addiction, regardless of the specific sedative used.
Most prescription sedatives are controlled substances. Under the federal Controlled Substances Act, sedatives are categorized into one of three schedules based on their accepted medical use and potential for misuse:
- Schedule II – the most tightly controlled prescription sedatives, including some barbiturates such as pentobarbital and secobarbital.
- Schedule III – moderate-risk sedatives, including certain barbiturate combination drugs.
- Schedule IV – lower-risk but still controlled sedatives, including most benzodiazepines (Xanax, Valium, Ativan, Klonopin) and the Z-drug sleep aids (Ambien, Lunesta, Sonata).
This classification means doctors must follow specific prescribing rules, pharmacies must track dispensing, and possessing these drugs without a valid prescription is a federal crime. Scheduling does not eliminate the risk of dependence or addiction; it reflects an attempt to balance medical usefulness against potential harm.2
How Sedatives Affect the Brain
Sedatives affect the brain by enhancing the activity of gamma-aminobutyric acid (GABA), a neurotransmitter that slows down nervous system activity, promoting a calming effect.
This reduction in brain excitability can produce feelings of relaxation, sedation and for some, euphoria or emotional numbing. For people coping with anxiety, trauma or pain, using sedatives to self-medicate may provide temporary relief. Still, it can also increase the risk of misuse and, over time, lead to dependence and addiction.
Common Types of Sedative Drugs
The sedative-hypnotic family covers several prescription drug classes that all calm brain activity through the GABA system. The most commonly misused are benzodiazepines, non-benzodiazepine sleep aids (Z-drugs), and barbiturates. Xylazine, a veterinary tranquilizer, has also moved into the illicit drug supply and behaves like a sedative even though it is not approved for human use.
Multiple drug classes fall under the category of being a CNS depressant. Along with sedatives, there are tranquilizers and hypnotics. While they differ in potency, duration and medical use, they share similar risks.
Sedatives, Hypnotics, and Anxiolytics: How the Terms Differ
The words “sedative,” “hypnotic,” “anxiolytic,” and “tranquilizer” are often used interchangeably, but each describes a slightly different effect on the brain. Most drugs in this family produce more than one of these effects depending on the dose, which is why clinicians group them together as the sedative-hypnotic-anxiolytic class.
| Term | What it primarily does | Example drugs |
|---|---|---|
| Sedative | Lowers excitement and produces calm at lower doses | Diazepam (Valium), phenobarbital |
| Anxiolytic | Reduces anxiety specifically, at sub-sedative doses | Alprazolam (Xanax), lorazepam (Ativan) |
| Hypnotic | Promotes or sustains sleep, usually at higher doses | Zolpidem (Ambien), temazepam (Restoril) |
| Tranquilizer (minor) | Older term, often used for anxiolytic benzodiazepines | Chlordiazepoxide (Librium), diazepam |
| Tranquilizer (major) | Antipsychotic drugs. not in the sedative-hypnotic class despite the name | Haloperidol, chlorpromazine |
The same benzodiazepine can be called an anxiolytic at one dose and a hypnotic at a higher dose. “Major tranquilizers” is an older name for antipsychotics and is not part of the sedative-hypnotic family, even though the word “tranquilizer” sounds similar.
Benzodiazepines
Prescription benzodiazepines are widely used to treat anxiety and panic disorders due to their fast-acting calming effects on the central nervous system. Benzodiazepines are typically recommended for limited and carefully monitored use, as misuse can lead to potential dependence. Benzodiazepines are typically recommended for limited and carefully monitored use.
Commonly prescribed benzodiazepines include:

Sleeping Pills
Non-benzodiazepine sleep aids, often referred to as “Z-drugs,” are a class of sedatives commonly prescribed to treat insomnia. Medications like Ambien, Lunesta and Sonata work by targeting GABA receptors in the brain, like benzodiazepines, to promote relaxation and help initiate sleep. Misusing them can lead to potentially life-threatening consequences.
Although they are typically marketed as safer alternatives to benzodiazepines, Z-drugs carry a risk of tolerance, dependence, and misuse. If you take them for a long time, you may need higher doses to achieve the same sleep effects, and stopping suddenly can lead to rebound insomnia or withdrawal symptoms.

Barbiturates
Barbiturates are an older class of sedative-hypnotic drugs that were widely prescribed for anxiety and sleep in the early-to-mid 20th century, before benzodiazepines took over most of that role. They are still used today for specific medical purposes, including seizure control, anesthesia, and some headache treatments.
Commonly prescribed barbiturates include:
- Phenobarbital (Luminal)
- Pentobarbital (Nembutal)
- Butalbital (Fiorinal, Fioricet)
- Secobarbital (Seconal)
Barbiturates carry a higher overdose risk than benzodiazepines because the gap between a therapeutic dose and a lethal dose is narrow, and the body adapts unevenly to repeated use. Mixing barbiturates with alcohol, opioids, or other CNS depressants greatly raises the risk of respiratory failure.
Withdrawal from barbiturate dependence is medically serious and can include seizures and delirium, which is why anyone considering stopping a long-term barbiturate prescription should taper under medical supervision rather than quitting abruptly.

Other Sedatives (Xylazine)
One growing concern is xylazine, commonly known as “tranq.” This substance, which is FDA-approved for use in veterinary medicine only, has increasingly been found mixed with street drugs like fentanyl.
It produces strong sedative effects, including extreme drowsiness, slowed breathing and reduced heart rate. However, it also carries severe physical side effects, such as dangerous drops in blood pressure and with repeated use the development of painful skin ulcers and tissue damage.
One reason that xylazine is so dangerous is that it does not respond to standard opioid overdose reversal medications like Narcan. Because it is not an opioid, naloxone cannot reverse its sedative effects, making overdoses more difficult to treat and increasing the risk of fatal outcomes. This is especially true when combined with opioids that further suppress breathing.

Opioids and Opiates
A Note on Opioids
Opioids and opiates such as fentanyl, oxycodone, and heroin are not typically classified as sedatives, even though they share some overlapping effects on the brain. Like sedatives, opioids slow breathing and produce drowsiness, but they act primarily on opioid receptors rather than the GABA system that sedatives target.
This distinction matters in two practical ways:
- First, the rising rate of fatal overdoses involving opioids and sedatives taken together is one of the most dangerous polysubstance patterns in the country today. Both classes suppress breathing, and the combined effect can be lethal at doses each drug would tolerate alone.
- Second, opioid overdose responds to naloxone (Narcan), while sedative overdose does not, which means the right emergency response depends on knowing what was taken.
Opioid misuse is associated with a high risk of overdose, especially when combined with other sedatives like benzodiazepines or alcohol.

Signs and Symptoms of Sedative Abuse
The signs of sedative misuse usually show up first as a slow change in behavior or daily functioning, not a dramatic single event. Physical signs include drowsiness, slurred speech, and poor coordination, while behavioral signs include secrecy, mood changes, and running out of medication early. Clinicians use the DSM-5-TR criteria for sedative, hypnotic, or anxiolytic use disorder to make a formal diagnosis.
Signs and symptoms of sedative abuse do not appear overnight; they progress and worsen the longer you use them. While symptoms of abuse vary from person to person, they often affect your behavior, physical health and overall functioning.
Physical Warning Signs
Physical warning signs of sedative abuse often reflect the drugs’ depressant effects on the central nervous system.
Common indicators include:
- Changes in physical appearance
- Pupils appear small
- Drowsiness
- Changes in appetite
- Changes in weight
- Intense flu-like symptoms
A key indicator of physical dependence is the presence of withdrawal symptoms between doses. This may include symptoms such as nausea and vomiting, elevated blood pressure, heart rate and body temperature, hallucinations, hypersensitive reflexes, anxiety or restlessness, insomnia, tremors or shaking, sweating and in severe cases, seizures.
Behavioral and Psychological Signs
Behavioral and psychological changes are often some of the most noticeable signs of sedative abuse.
Behavioral warning signs may include:
- Change in attitude and/or personality
- Tendency to avoid contact with family and/or friends
- Change in friends, work, school, activities, etc.
- Poor performance at work or school
- Isolation or acting in a secretive manner
- Moodiness, irritability, nervousness, giddiness
- Tendency to steal
Doctor shopping is another indicator of sedative abuse. Doctor shopping is when a person visits multiple doctors to try to obtain multiple prescriptions. Although advanced record-sharing databases help prevent this, some people will still travel hundreds of miles to obtain the medicines they desire.
Psychological and cognitive effects may include:
- Memory problems or frequent forgetfulness
- Difficulty concentrating or impaired thinking
- Confusion or disorientation
- Mood swings, including irritability or sudden calmness
- Depression or emotional numbness
Recognizing the signs of sedative abuse is important for early intervention. This helps to prevent misuse from progressing into severe dependence or addiction and allows individuals and loved ones to seek support before the problem worsens.
How Sedative Use Disorder Is Diagnosed (DSM-5-TR)
A formal diagnosis of sedative addiction comes from a licensed clinician using the criteria for sedative, hypnotic, or anxiolytic use disorder in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). A clinician looks for a pattern of sedative use that causes clinically significant impairment or distress over a 12-month period, with at least two of the following 11 features:
- Taking more sedatives than intended or for longer than intended
- Persistent wish, or unsuccessful efforts, to cut down or stop
- A great deal of time spent obtaining, using, or recovering from sedatives
- Cravings or strong urges to use
- Sedative use that interferes with major roles at work, school, or home
- Continued use despite social or interpersonal problems
- Important activities given up or reduced
- Use in physically hazardous situations
- Use continued despite known physical or psychological harm
- Tolerance (needing more to get the same effect)
- Withdrawal symptoms or use of sedatives to relieve withdrawal
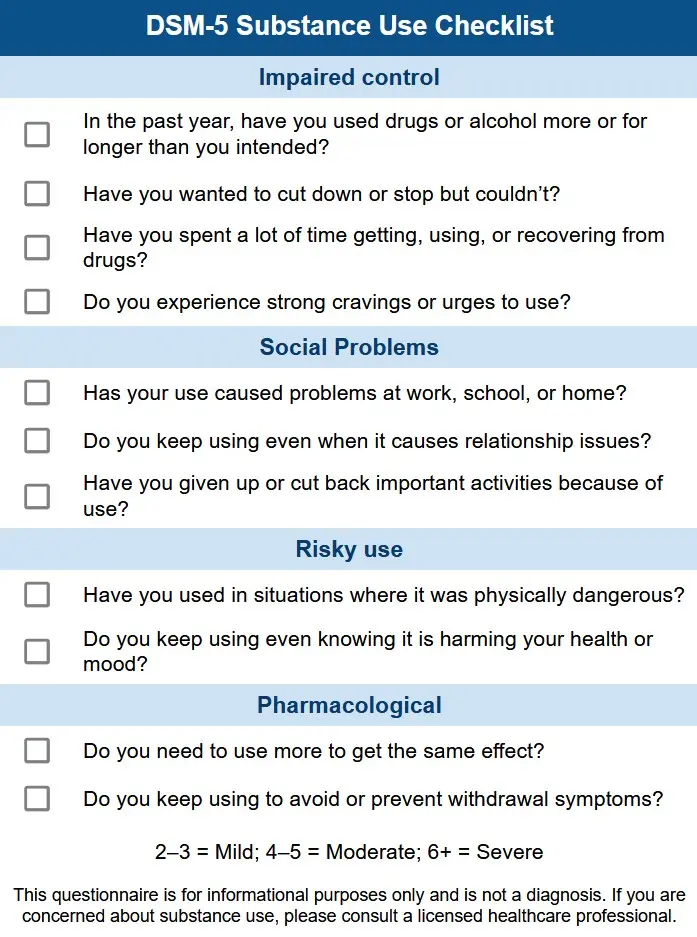
Severity is rated as mild (two or three criteria), moderate (four or five), or severe (six or more). Tolerance and withdrawal that occur under appropriate medical supervision are generally not counted toward the diagnosis on their own.5
The Dangers and Risks of Sedative Addiction
Chronic sedative misuse can lead to severe health risks and life-threatening outcomes, especially when mixed with other substances. Long-term use affects brain function and can lead to dependence, addiction and overdose.
Overdose and Polysubstance Abuse
Overdose and polysubstance abuse are among the most dangerous risks associated with sedative use.
Combining sedatives with other CNS depressants, especially alcohol or opioids, greatly increases the likelihood of a life-threatening overdose, because each substance on its own can slow brain activity, leading to severe respiratory depression.
More than 9 in 10 benzodiazepine-involved overdose deaths in the United States also involve an opioid, based on CDC drug overdose surveillance data.6 This is one of the clearest signals of how dangerous mixing sedatives with opioids has become.
Because the brain’s ability to regulate vital functions is impaired, the body may not respond in time to restore normal breathing, resulting in a fatal outcome.

Long-Term Health Consequences
Long-term sedative use can lead to lasting and sometimes irreversible health consequences.
Prolonged misuse is associated with the following:
- Memory problems
- Slow thinking
- Difficulty concentrating
- Rebound anxiety
- Insomnia
In addition, chronic sedative use can place strain on the body, contributing to cardiovascular issues such as low blood pressure, irregular heart rate and overall reduced physical stability, further increasing the risk of long-term health complications.
Sedative Withdrawal and Detoxification
Sedative withdrawal can be one of the most medically dangerous forms of substance withdrawal, with seizures and severe autonomic symptoms among the possible complications. Symptoms usually begin within 1 to 4 days of the last dose, peak in the first week, and may continue at a lower intensity for several weeks. Because of these risks, sedative detox is almost always done under medical supervision with a gradual taper rather than abrupt cessation.
Common withdrawal symptoms include:
- Anxiety and restlessness
- Insomnia or disturbed sleep
- Tremors or shaking
- Rapid heart rate or palpitations
- Sweating
- Nausea or vomiting
- Confusion or agitation
If not properly managed, you may experience severe withdrawal symptoms. Pharmacological tapering options are available under medical supervision.
Sedative Withdrawal Timeline
Sedative withdrawal unfolds in phases that vary by the specific drug, the dose, how long it was used, and individual factors like age and overall health. Short-acting sedatives such as alprazolam (Xanax) typically produce earlier and sharper withdrawal than longer-acting ones like diazepam (Valium) or phenobarbital, but the broad timeline below applies across the class.
| Phase | Timing | What to expect |
|---|---|---|
| Early symptoms | 6 to 24 hours after the last dose for short-acting drugs; 1 to 4 days for long-acting drugs | Rising anxiety, restlessness, trouble sleeping, sweating, racing heart |
| Peak | Days 2 to 7 for short-acting drugs; days 5 to 14 for long-acting drugs | Tremor, nausea, elevated blood pressure, possible seizures, hallucinations, or delirium in severe cases |
| Subacute | Weeks 2 to 4 | Lingering insomnia, anxiety, irritability, and physical discomfort that gradually ease |
| Protracted (PAWS) | Weeks to months | Slow recovery of sleep, mood, and cognitive function; cravings may come and go |
Seizures are the single most dangerous complication of sedative withdrawal and are most likely during the peak phase. Anyone with a long history of high-dose sedative use, prior withdrawal seizures, or co-occurring alcohol use is at especially high risk.7 This is the medical reason an unsupervised “cold turkey” attempt at home is not safe.
The Importance of Medical Detox
The importance of medical detox cannot be overstated for individuals with severe sedative addictions.
Attempting to quit “cold turkey” can be extremely dangerous due to the risk of life-threatening withdrawal symptoms. Medical detox provides a structured, supervised approach that involves a tapering schedule, where doses are slowly decreased under professional monitoring.
This method helps to:
- Minimize severe withdrawal symptoms
- Reduce the risk of seizures and other complications
- Make the detox process more manageable and safer
- Provide immediate medical support if complications arise
By using medical detox, individuals can begin recovery in a way that prioritizes safety and long-term success. After detox, individuals can transition to an appropriate level of care to continue their recovery journey.

Sedative Addiction Treatment
Sedative addiction treatment usually starts with medically supervised detox, followed by inpatient or outpatient rehab and ongoing recovery support. There are no FDA-approved medications specifically for sedative use disorder, so treatment leans on behavioral therapies like cognitive behavioral therapy, contingency management, and group counseling. Care plans are most effective when they also address co-occurring conditions such as anxiety, depression, or trauma that may have driven sedative use in the first place.
Inpatient vs Outpatient Programs
Inpatient vs. outpatient programs offer different levels of care for sedative addiction treatment, with each suited to varying levels of severity and individual needs.
Inpatient addiction programs provide 24/7 care in a structured environment where individuals receive medical support during withdrawal and comprehensive addiction treatment.
Intensive outpatient programs (IOPs) and partial hospitalization programs (PHPs) offer greater flexibility, allowing patients to live at home while attending regular therapy and counseling sessions. Some outpatient programs can be done via telehealth. Both programs offer more intensive care than standard outpatient care.

Therapeutic Approaches in Recovery
Evidence-based therapies play a key role in sedative addiction treatment by addressing the underlying thoughts, emotions and behaviors that drive misuse.
Commonly used therapies include:
- Cognitive behavioral therapy (CBT) – Helps patients identify triggers, challenge harmful thought patterns and develop healthier coping strategies
- Dialectical behavioral therapy (DBT) – Focuses on emotion regulation, distress tolerance and interpersonal effectiveness
- Motivational interviewing (MI) – Encourages personal motivation and commitment to change
- Contingency management (CM) – Uses positive reinforcement to support abstinence and treatment adherence
- Group and family therapy – Provides social support, accountability and improved communication skills
Treating co-occurring mental health disorders is also critical, as sedatives are often misused to self-medicate anxiety, depression, or trauma. Integrated dual diagnosis treatment addresses both addiction and underlying psychological conditions, improving recovery outcomes and reducing relapse risk.
Frequently Asked Questions
The questions below come up most often from people researching sedative addiction for themselves or a loved one. The answers are intended as a starting point, not a substitute for a conversation with a clinician who can review your specific situation.
While some sedatives have higher abuse potential than others, nearly all CNS depressants carry a risk of physical dependence and addiction. Even certain sleep aids can lead to tolerance, withdrawal, and compulsive use when taken for extended periods.
Combining sedatives with alcohol amplifies their CNS depressant effects, slowing brain and body functions more than either substance alone. This can lead to dangerously slowed or stopped breathing, loss of consciousness, coma and even fatal overdose.
No. Because xylazine is a non-opioid sedative, naloxone (Narcan) cannot reverse its effects. This makes overdoses involving xylazine especially dangerous, as standard opioid overdose treatments are ineffective.
Individuals exposed to xylazine may experience severe sedation, slowed breathing and other life-threatening symptoms, requiring immediate medical attention and supportive care.
For most people, the acute phase of sedative withdrawal lasts 1 to 2 weeks, with peak symptoms typically falling between days 2 and 7 for short-acting drugs and days 5 to 14 for long-acting drugs. A milder protracted phase, sometimes called post-acute withdrawal, can continue for weeks to months. The exact timeline depends on the specific sedative, dose, and length of use.
Dependence is a physical adaptation: the body has become used to the drug and produces withdrawal symptoms when the drug is reduced or stopped. Addiction is a broader pattern that also includes compulsive use, cravings, and continued use despite harm. A person can be physically dependent on a properly prescribed sedative without meeting criteria for addiction, although dependence does raise the risk of progressing to addiction over time.
For most people taking sedatives regularly, no. Abrupt cessation of benzodiazepines, barbiturates, or long-term Z-drug use can trigger severe withdrawal symptoms including seizures, hallucinations, and dangerously high blood pressure. Quitting safely usually requires a gradual taper supervised by a clinician, sometimes within a medical detox program.
Yes. The path to a sedative use disorder often starts with a legitimate prescription, and treatment is designed to address that reality. Clinicians work with people to taper off the original prescription safely, address the underlying condition (often anxiety, insomnia, or trauma) that led to the prescription, and offer non-addictive alternatives or therapies where appropriate.
Find Treatment Near You
Not sure where to start? Use our rehab center directory to find top-rated treatment centers across the U.S., filtering by location, level of care, insurance and specialized programs offered.
If you prefer to talk to someone, call today. A professional can explain treatment options and verify if your insurance covers rehab.
Call A Treatment Provider
For a conversation about what treatment options are available to you.
Make a Call
Featured Facilities Near You
Finding facilities near you…
Finding facilities near you…
Finding facilities near you…
References
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2024 National Survey on Drug Use and Health. HHS Publication No. PEP25-07-007, NSDUH Series H-60. Center for Behavioral Health Statistics and Quality, SAMHSA; 2025. Accessed May 19, 2026. https://www.samhsa.gov/data/report/2024-nsduh-annual-national-report
- U.S. Drug Enforcement Administration. Drug Scheduling. DEA Diversion Control Division. Accessed May 19, 2026. https://www.dea.gov/drug-information/drug-scheduling
- U.S. Food and Drug Administration. FDA alerts health care professionals of risks to patients exposed to xylazine in illicit drugs. FDA Drug Safety Communication. November 8, 2022. Updated November 27, 2024. Accessed May 19, 2026. https://www.fda.gov/drugs/drug-safety-and-availability/fda-alerts-health-care-professionals-risks-patients-exposed-xylazine-illicit-drugs
- Sansone RA, Sansone LA. Doctor shopping: a phenomenon of many themes. Innovations in Clinical Neuroscience. 2012;9(11-12):42-46. Accessed May 19, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC4553644/
- American Psychiatric Association. Sedative, Hypnotic, or Anxiolytic Use Disorder. In: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Association Publishing; 2022.
- Liu S, O’Donnell J, Gladden RM, McGlone L, Chowdhury F. Trends in Nonfatal and Fatal Overdoses Involving Benzodiazepines — 38 States and the District of Columbia, 2019-2020. MMWR Morbidity and Mortality Weekly Report. 2021;70(34):1136-1141. Centers for Disease Control and Prevention. Accessed May 19, 2026. https://www.cdc.gov/mmwr/volumes/70/wr/mm7034a2.htm
- National Institute on Drug Abuse. Prescription CNS Depressants DrugFacts. National Institutes of Health, U.S. Department of Health and Human Services; updated March 2018. Accessed May 19, 2026. https://nida.nih.gov/publications/drugfacts/prescription-cns-depressants





