
































































































Stimulants are substances that speed up brain activity and increase energy and alertness. Legal and illegal stimulants can be misused, leading to stimulant addiction, also called stimulant use disorder. In 2024, an estimated 4.3 million Americans aged 12 or older met criteria for a central nervous system stimulant use disorder, according to the Substance Abuse and Mental Health Services Administration.1
This article covers the different types of stimulants, their short- and long-term risks, and stimulant withdrawal symptoms. It also covers what stimulant addiction treatment entails, including levels of care, evidence-based therapies, and relapse prevention, and what to look for when choosing a treatment program.
Key Points
- Stimulants speed up the central nervous system, increasing energy, alertness, and dopamine release in the brain’s reward pathway.
- Common stimulants include cocaine, methamphetamine, and prescription medications like Adderall, Ritalin, Vyvanse, and Concerta.
- Stimulants were involved in 59% of US drug overdose deaths between January 2021 and June 2024, according to the CDC.
- About 4.3 million Americans had a central nervous system stimulant use disorder in 2024, per SAMHSA’s NSDUH.
- No FDA-approved medications exist for stimulant use disorder; CBT and contingency management are first-line treatments.
- Withdrawal is rarely medically dangerous but carries real depression and suicide risk; medical monitoring is recommended.
In This Article:
- What are stimulants?
- Understanding stimulant addiction (stimulant use disorder)
- Stimulant withdrawal and detox
- Evidence-based treatment approaches
- Levels of care for stimulant addiction
- Integrated and specialized programs
- Holistic and complementary supports
- Relapse prevention and long-term recovery
- Choosing a stimulant addiction treatment program
- FAQs about treating stimulant addiction
- Find treatment near you
What Are Stimulants?
Stimulants are often called “uppers” because they make the user more alert, attentive, and energetic. They include legal substances like caffeine and nicotine, illegal substances like cocaine and methamphetamine, and prescription drugs used to treat conditions such as ADHD and narcolepsy. People use stimulants for performance enhancement, medical reasons, and recreational purposes.
Caffeine is the most commonly used stimulant in the world. Other examples include amphetamines, cocaine, and prescription stimulants such as Adderall, Ritalin, Vyvanse, and Concerta.
Illicit Stimulants (Cocaine, Methamphetamine, Bath Salts)
- Cocaine exists in powder form, with street names that include “coke,” “snow,” and “blow.” Cocaine is often snorted, dissolved in water and injected intravenously, or smoked as crack cocaine.
- Methamphetamine (meth) is synthetic, meaning it is made in a lab. Sold on the street in rock or crystal form, meth is often called “crystal meth” or “ice.”
- Synthetic cathinones are lab-made substances that create effects similar to cocaine and meth. Often called “bath salts,” they are snorted, taken orally, smoked, or injected intravenously.
- Pink cocaine (sometimes called “tusi”) is rarely actual cocaine. It is usually a pink-dyed mixture of substances like ketamine, MDMA, and caffeine, with unpredictable composition.
Typical illicit stimulant use follows a binge-and-crash pattern. People use large doses over a short period, which causes a “crash” involving depression, hunger, and the need to rest for several days. This pattern causes a short, sudden spike in dopamine levels.
Dopamine is a chemical involved in experiencing pleasure, and the surge reinforces stimulant use. Binging causes tolerance quickly, heavier subsequent binges, more severe crashes, and an intense craving for the stimulant.
Prescription Stimulants (Adderall, Ritalin, Vyvanse, Concerta)
Because stimulants increase attention and alertness, they are often prescribed for ADHD and narcolepsy. Taken exactly as prescribed for a therapeutic purpose, prescription stimulants like Adderall, Ritalin, Vyvanse, and Concerta can work well in controlling these conditions.
However, some people misuse these medications to focus on schoolwork, suppress appetite, or stay awake longer. Prescription stimulants can also be crushed and snorted or dissolved and injected, which produces a faster, more intense effect and increases addiction risk.
Intravenous use carries health risks like the transfer of bloodborne viruses from contaminated needles. Some people engage in diversion by selling, sharing, or trading their prescription stimulants. Others turn to illicit stimulants when their prescription runs out or is no longer available.
Understanding Stimulant Addiction (Stimulant Use Disorder)
Stimulant use disorder is a clinical diagnosis describing problematic stimulant use that causes significant impairment or distress.7 Stimulants are addictive because they cause immediate euphoria and prolonged alertness, which reinforces use and causes cravings. Repeated use rewires the brain’s reward system, making cravings persistent even after stopping.
4.3 Million Americans
In 2024, an estimated 4.3 million people aged 12 or older had a central nervous system stimulant use disorder, per SAMHSA’s NSDUH.
No FDA-Approved Medications
No medications are currently approved by the FDA to treat stimulant use disorder. Behavioral therapies remain first-line care.
Why Stimulants Are Addictive
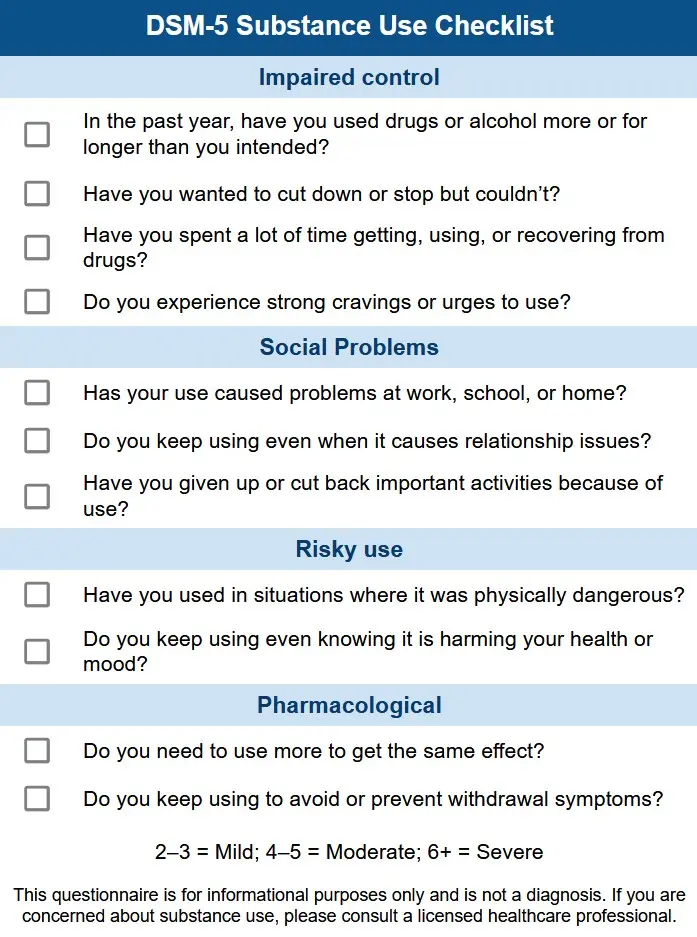
According to DSM-5 criteria, a stimulant use disorder may be present when two or more of the following occur within a 12-month period:7
- Stimulant is used in larger amounts or for longer than intended
- Multiple unsuccessful attempts to stop the use
- Continued use despite it causing interpersonal problems
- Continued use despite it contributing to a physical or mental condition
- Repeated use in dangerous situations
- Responsibilities are neglected because of use
- Significant time is spent acquiring, using, or recovering from the effects of stimulants
- Strong cravings for stimulants
- Giving up important activities to use
- Tolerance
- Withdrawal
What Are the Risks of Stimulant Use?
Using prescription or illicit stimulants carries side effects and is often associated with withdrawal symptoms and risks to physical and mental health. Severity varies depending on the combination of substances used, route of administration, potency, dosage, and prior use history. Effects can be short-term or long-term.
Short-Term Effects of Stimulant Use
The following side effects can appear within hours or days and are usually experienced temporarily even with controlled use of stimulants:
- Accelerated heart rate
- Vasoconstriction
- Increased blood pressure
- Elevated body temperature
- Panic attacks
- Paranoia
- Hostility
- Fatigue
- Depression
- Changes in appetite leading to weight loss
- Impaired memory
Long-Term Effects of Using Stimulants
Using stimulants more frequently and in higher doses for a prolonged period can lead to addiction or stimulant use disorder. There are many long-term health problems related to chronic stimulant misuse, including:
Changes to the Brain
Stimulant use disorder affects long-term memory and the ability to learn new things. It also triggers the addiction process, driving cravings and ongoing drug use.
Psychosis and Mental Health Effects
Long-term stimulant use can cause behavioral changes, paranoia, hallucinations, and delusions. It can also worsen existing mental health conditions like bipolar disorder.
Cardiovascular Strain
Stimulants strain the heart and raise the long-term risk of strokes and heart attacks. Elevated body temperature can also lead to hyperthermia.
Disrupted Brain Chemistry
Effects on dopamine and other hormone levels can persist long after stimulant use stops. The brain may struggle to produce dopamine naturally, leaving the person anxious, paranoid, and chronically depressed.
Risk of Overdose and Death
It is possible to overdose on stimulants with severe and life-threatening consequences. People who use stimulants in excessive quantities risk seizures, hyperthermia, hypertensive emergencies, stroke, cardiac arrest, and death. The risk of overdose applies to both prescribed and illicit stimulants.
According to the National Institute on Drug Abuse, drug overdose deaths involving psychostimulants (such as methamphetamine) rose from 5,716 in 2015 to 34,855 in 2023, while cocaine-involved overdose deaths reached 29,449 in the same year.3 A large share of stimulant-involved deaths now also involve illegally manufactured fentanyl, which has become a primary driver of stimulant overdose mortality.
Stimulants were involved in 59% of US drug overdose deaths from January 2021 to June 2024, according to CDC MMWR.
Nearly 70% of stimulant-involved overdose deaths in 2023 also involved illegally manufactured fentanyl, per NIDA.
Provisional CDC data show overall stimulant-involved overdose deaths began declining in 2024 and continued falling in 2025 alongside opioid deaths, but totals remain well above pre-2015 levels.8
Stimulant Withdrawal and Detox
Stimulant withdrawal is rarely physically dangerous in the way alcohol withdrawal or benzodiazepine withdrawal can be, but the psychiatric symptoms are serious. Acute symptoms typically peak within the first week and can include severe depression, fatigue, and suicidal ideation that warrant clinical monitoring.
Common Stimulant Withdrawal Symptoms and Severity
When prolonged stimulant use is suddenly discontinued, it can cause:
- Depression
- Fatigue
- Sleep problems
- Increased appetite
- Unusually slow or fast movement
- Intense cravings (a major cause of relapse)
- Suicidal ideation, the most serious potential symptom, which can peak from 24 to 72 hours after last use
Day-by-Day Withdrawal Timeline
The course of stimulant withdrawal varies by the specific drug, dose, and duration of use, but generally follows this pattern:
| Stage | What to expect |
|---|---|
| First 24 hours | The “crash,” or acute withdrawal, begins. Fatigue, depression, and intense cravings can set in quickly. |
| Days 2 to 7 | Acute withdrawal continues. Suicidal thoughts may begin in the first one to two weeks and warrant clinical monitoring. |
| Days 3 to 4 | Hypersomnia and appetite surge are common. People often sleep heavily and eat more than usual. |
| Weeks to months later | Protracted withdrawal can occur with some stimulants like methamphetamine, including persistent depression, fatigue, and loss of interest. |
Stimulant Detox: Safety, Monitoring, and Suicide Risk
Detoxing from stimulants is generally not medically dangerous, and medications are rarely required. Medical detox under provider supervision can still be helpful depending on the situation, particularly when psychiatric symptoms are severe.
Inpatient detox may be needed if the person:
- Has severe depression or suicidal ideation
- Has psychosis
- Has other substance use disorders
- Is pregnant
Medical detox involves monitoring vital signs, following sleep aid protocols, and administering medications like antidepressants when appropriate.
Managing Acute Psychiatric Complications
Medications may also be used to treat psychiatric complications from stimulant use. Benzodiazepines may be prescribed in cases of severe agitation. Antipsychotics may be prescribed for stimulant-induced psychosis.
For cases of suicidal ideation or severe depression, safety planning and connection with medication trials may also be appropriate. The ASAM/AAAP Clinical Practice Guideline on Stimulant Use Disorder recommends close monitoring during early withdrawal.4
Call A Treatment Provider
For a conversation about what treatment options are available to you.
Make a Call
Evidence-Based Treatment Approaches
Because no FDA-approved medications exist for stimulant use disorder, behavioral therapies and psychosocial interventions are the foundation of treatment. The ASAM/AAAP Clinical Practice Guideline identifies contingency management, cognitive-behavioral therapy, and the Matrix Model as evidence-based first-line approaches.4
Behavioral Therapies: CBT, Contingency Management, Matrix Model
Cognitive-behavioral therapy (CBT) works to identify and change unhelpful thoughts linked to use and to develop healthy coping strategies. CBT has been shown to reduce the number of stimulant relapse episodes.
Contingency management (CM) is another evidence-based therapy commonly used for stimulant addiction. CM involves providing prizes or vouchers for meeting specific goals such as negative urine drug screens. It has the strongest evidence base of any psychosocial intervention for stimulant use disorder.4
The Matrix Model integrates CBT, contingency management, drug urinalysis, and family education into a 16-week manualized format. It includes individual therapy, skills and social support groups, and family education sessions, which help family members better understand their loved one’s struggle and how to support them.

Motivational Interviewing and Community Reinforcement
Motivational interviewing (MI) is another type of therapy often part of addiction treatment. A person with addiction often deals with inner conflicts about use. They may know it is not healthy, but the perceived short-term benefits take over. MI helps the person work through these conflicts and move closer to making a healthy change.
The Community Reinforcement Approach (CRA) helps people build a healthy, pleasurable lifestyle that reinforces recovery. This includes training in problem solving, communication skills (such as substance refusal), job skills, and building sober social activities. CRA is especially effective in rural settings.
Emerging Pharmacotherapies and Clinical Trials
There are currently no medications approved by the US Food and Drug Administration for stimulant use disorder. However, several clinical trials are in progress. Topiramate has been shown to be better than placebo at increasing the number of days of cocaine abstinence.
The ADAPT-2 trial, published in the New England Journal of Medicine, found that a combination of extended-release injectable naltrexone and oral bupropion produced a treatment response in more than 13% of participants with moderate or severe methamphetamine use disorder, compared with about 2.5% of those on placebo.5
A separate placebo-controlled study published in JAMA Psychiatry found mirtazapine helped reduce methamphetamine use among men who have sex with men, with effects sustained for several months after the intervention period.6
Long-acting injectable psychostimulants like extended-release amphetamine are also being investigated for agonist therapy in cocaine and methamphetamine use disorders.
Digital Therapeutics and Telehealth Delivery
Apps can also help facilitate recovery with features like CBT exercises, craving trackers, and push notifications. Telehealth on privacy and security-vetted platforms has expanded access and allowed for flexible scheduling, particularly for people in rural or underserved areas.

Levels of Care for Stimulant Addiction
Stimulant addiction treatment is delivered across a continuum of care, from 24/7 residential programs to weekly outpatient sessions and long-term aftercare. The right level depends on addiction severity, co-occurring conditions, home environment, and prior treatment history.
| Level of care | Best for | Typical duration |
|---|---|---|
| Inpatient / residential rehab | Severe addiction, co-occurring mental health conditions, unstable home environment | 28 to 90 days |
| Partial hospitalization (PHP) | Daytime structure with home support; step-down from inpatient | 2 to 4 weeks typical |
| Intensive outpatient (IOP) | Stable home environment; need to work or attend school | 8 to 12 weeks typical |
| Standard outpatient | Mild addiction or step-down from more intensive care | 3 to 6 months or longer |
| Aftercare and sober living | Long-term recovery support after primary treatment | Variable; often 3 to 12 months |
Inpatient and Residential Rehab
Inpatient or residential rehab involves living at the treatment facility and receiving care and supervision around the clock. Treatment is structured with individual and group therapy, drug education, case management services like vocational rehab, and health-promoting activities.
Services are provided by a multidisciplinary team that may include doctors, nurses, psychiatrists, psychologists, case managers, and therapists. A typical inpatient stay lasts 28 to 90 days and is suitable for someone with severe addiction, co-occurring mental health conditions, or a home environment that is not supportive of recovery.

Partial Hospitalization and Intensive Outpatient Programs (IOP)
Partial hospitalization programs (PHP) and intensive outpatient (IOP) programs involve living at home while commuting to services. These programs typically involve 20 to 30 hours of services per week for PHP and 9 to 19 hours for IOP.
PHP and IOP programs have comparable outcomes to inpatient rehab at a lower cost. They are also suited for those who have a home environment supportive of recovery or who need to work or attend school while in treatment.

Standard Outpatient Counseling and Tele-IOP
Standard outpatient counseling consists of one to three hours per week of individual or group therapy. This is often a fit for someone with a mild addiction or as a step-down program after completing a more intensive rehab program.
IOP via telehealth is also available, with urine testing done via mail-in kits to make treatment more accessible for people who cannot easily reach a clinic.
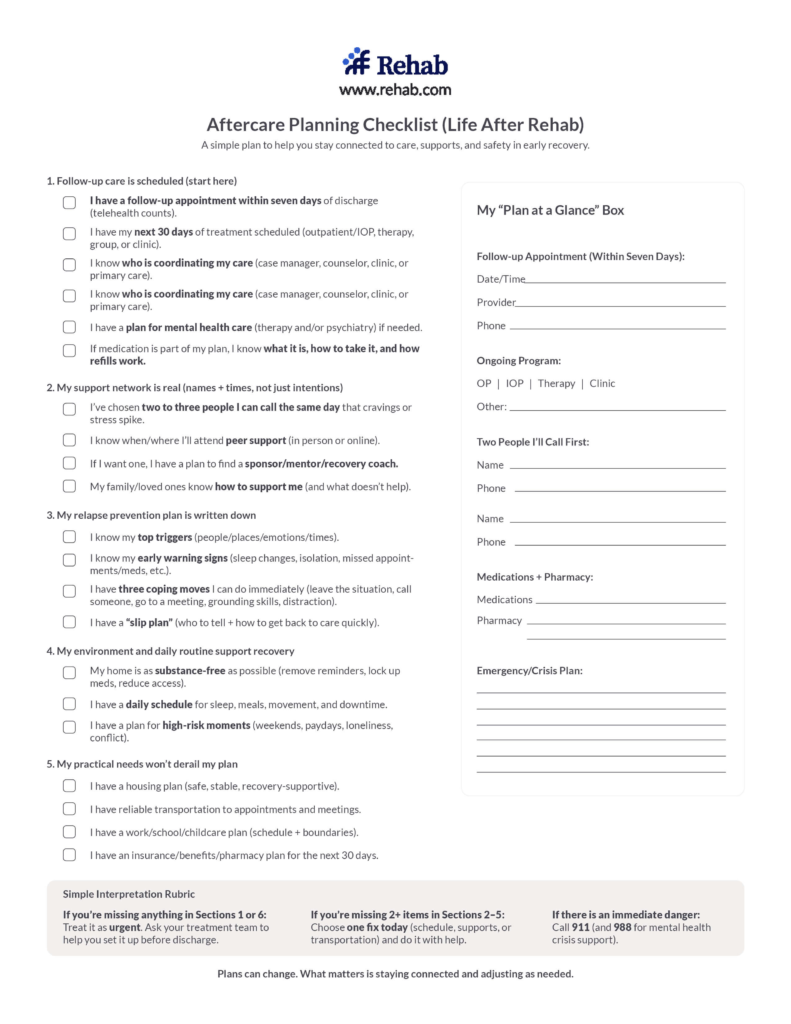
Aftercare Planning and Step-Down Continuum
Aftercare helps maintain progress made in rehab and reduce the risk of relapse. The recovery continuum steps down in intensity over time. Sober living homes are a higher level of aftercare; alumni groups and peer support meetings are a lower level. Group attendance may decrease in frequency as sobriety continues.
Key performance indicators of aftercare include attendance, consistent employment, and negative drug screens.

Integrated and Specialized Programs
Integrated and specialized programs may better fit someone who has a stimulant use disorder along with other clinical or social needs. These programs address the conditions, identities, and life circumstances that affect treatment outcomes.
Dual Diagnosis (Mental Health and Stimulant Use)
If someone has a co-occurring disorder, meaning they have a mental health condition in addition to addiction, treating both concurrently increases chances of positive outcomes. Dual diagnosis treatment involves one treatment plan that integrates interventions for addiction and psychiatric conditions, including both therapy and medication management.
This is especially important for stimulant use disorder because mental health conditions like depression, anxiety, and bipolar disorder can drive stimulant use, and chronic stimulant use can worsen or unmask these conditions.
Gender-Responsive and LGBTQ+-Affirming Tracks
Challenges faced by gender and sexual minority populations can include intimate partner violence and stress related to discrimination. Having a safe space to discuss LGBTQ+ concerns encourages disclosure and engagement and reduces the risk of dropout.
Gender-responsive tracks for women and men also address gender-specific clinical and social factors, including trauma, parenting responsibilities, and workplace pressures.
Adolescent and Young Adult Treatment Considerations
Treatment success is more likely for adolescents and young adults when interventions match their developmental stage. Retention in these programs can be bolstered by gamified contingency management. It is also important for this population that treatment incorporates family and school elements to foster recovery support.
Culturally Tailored, Tribal, and Rural Services
Stimulant addiction programs that are tailored to specific cultures address the values and customs of that culture, which helps treatment retention and outcomes. Such programs may integrate traditional healing practices like sweat lodges and deliver treatment in the group’s native language.
For rural communities, mobile clinics and telehealth can help overcome geographic isolation and provider shortages.

Holistic and Complementary Supports
Holistic and complementary supports can help someone affected by stimulant addiction stabilize physically and emotionally during recovery. These approaches do not replace evidence-based treatment, but they reinforce it.
Exercise, Sleep, and Nutrition in Neuro-Recovery
Brain health is an important part of recovery because stimulant addiction affects neural functioning, which results in mood and circadian rhythm changes. Aerobic activity releases natural endorphins and boosts brain-derived neurotrophic factor (BDNF), a protein that supports neurotransmitter function. A high-protein, micronutrient-rich diet also helps repair BDNF function.
Mindfulness, Meditation, and Stress-Management Tools
Mindfulness-based stress reduction (MBSR) strategies can help individuals cope with cravings and manage their emotions. Activities like yoga and mindfulness meditation can help dissipate cravings and negative moods. Apps are also available that provide on-demand coping methods when experiencing cravings.

Peer-Led Recovery Groups (NA, SMART Recovery, Recovery Dharma)
Peer-led recovery groups can play a meaningful role in long-term recovery. Well-known peer groups include 12-step programs like Narcotics Anonymous (NA) and Cocaine Anonymous (CA).
Secular groups and groups suited to different philosophies are also available. SMART Recovery, which stands for Self-Management and Recovery Training, uses cognitive-behavioral tools. Recovery Dharma uses Buddhist practices and principles.
Benefits of peer recovery groups include feeling a sense of accountability to others and sharing experiences and coping ideas with people who have similar struggles. Meetings are increasingly available online to expand access and flexibility.

Family Engagement and the CRAFT Model
Community Reinforcement and Family Training (CRAFT) is a program that teaches family members how to positively reinforce their loved one’s healthy behaviors and encourage them to enter treatment when needed. CRAFT also teaches how to decrease enabling behaviors and improve the family’s overall well-being.
Relapse Prevention and Long-Term Recovery
Long-term recovery from stimulant use disorder is an ongoing process. Relapse prevention focuses on identifying and managing triggers, sustaining behavioral skills learned in treatment, and building a life that reinforces sobriety.
Identifying Triggers, Cravings, and High-Risk Situations
Recovery is an ongoing process of identifying and dealing with triggers and cravings. This includes internal cues (such as boredom or recalling the euphoria of past use) and external cues (such as parties or paydays). Keeping a diary of triggers can help control them.
Self-checks during cravings also help. The HALT check asks if you are Hungry, Angry, Lonely, or Tired so you can meet those underlying needs instead of turning to drugs or alcohol.
Contingency Management in Continuing Care
Contingency management can continue during recovery to help prevent relapse. This may include drug screens with results reported to a counselor. Low-cost prizes for negative screens can help maintain abstinence over time.
Building Recovery Capital: Housing, Employment, Social Networks
Long-term recovery also includes fostering a good quality of life. Efforts depend on individual needs and could involve vocational rehab, strengthening protective factors like social support, and engaging in activities that give meaning and purpose. These elements together are called recovery capital. A higher recovery capital score is associated with a greater chance of sustaining remission.
Monitoring, Drug Testing, and Recovery-Support Apps
Additional tools to deter relapse include smartphone apps that randomly alert you to submit a saliva sample for drug testing. Apps can also send CBT prompts to practice skills learned in therapy. Geofencing apps can alert you if you are close to a location that could trigger use.
Choosing a Stimulant Addiction Treatment Program
Choosing a treatment program is a high-stakes decision. Look for evidence-based care, transparent reporting, in-network insurance acceptance, and a clinical team experienced in stimulant use disorder specifically.
Accreditation, Licensure, Evidence-Based Track Records
Check a program’s website for transparency on its treatment retention and abstinence rates. Look for staff credentials and licensures. A quality facility will be licensed by its state and may also hold accreditation from CARF or The Joint Commission, two of the most recognized accrediting bodies in addiction treatment.
Insurance Verification, Sliding-Scale, and Financing Options
The cost of rehab is a valid concern. Check if a program accepts your insurance and whether the facility is in or out of network. The Affordable Care Act requires most insurance plans to provide coverage for addiction and mental health treatment.
Medicaid and TRICARE allow states flexibility in using telehealth and may have coverage for contingency management interventions. Facilities may also offer grants, sliding-scale fees, or payment plans. For more on coverage, see our guide to whether insurance covers rehab.

Questions to Ask Prospective Providers
Other factors that may affect treatment success include the average caseload of therapists, how often urine drug screens are conducted, whether the program offers services for family members, and whether alumni support is provided after treatment.
You can also ask if medication-assisted treatment (MAT) is available for any co-occurring opioid or alcohol use disorder, or if the program can provide referrals for stimulant pharmacotherapy clinical trials.
Telehealth vs. On-Site: Pros, Cons, and Suitability
Telehealth can yield outcomes similar to in-person treatment for mild to moderate stimulant addiction. Check whether a facility offers online rehab, especially if barriers like transportation or childcare make in-person services difficult.
However, when there is an unstable home environment, severe addiction, or significant co-occurring conditions, inpatient treatment is generally recommended.
FAQs About Treating Stimulant Addiction
No, stimulant addiction cannot be cured. It is a chronic yet manageable condition. Long term remission is possible. Remission rates improve with good recovery capital and treatment that lasts at least 90 days. Additionally, the brain can recover its plasticity over 12 to 18 months which also supports long-term recovery.
No, there are currently no FDA approved medications to treat stimulant use disorder. CM and CBT are the first line treatments. Several potential medications are in the third phase of their trials. Off label bupropion or mirtazapine are sometimes used for depressive symptoms in withdrawal.
Treatment initially lasts about three to four months. Ongoing monitoring and aftercare services that last 12 months or more are recommended. This helps sustain progress made in treatment and helps to prevent relapse. More time spent in treatment and aftercare can double your chances of sustaining abstinence. See more about how long treatment takes.
You can help a loved one refuse stimulants in a number of ways like encouraging them to seek professional help, avoiding enabling their behaviors, setting clear boundaries and providing drug-free social interactions. The CRAFT program can help your family develop these skills.
Find Treatment Near You
Rehab.com’s online directory can help you locate stimulant addiction treatment programs in your area. Enter your location and click “Find Care.” The search results can be filtered by level of care, program type, payment options, accreditations, amenities, and insurance.
Not sure where to start? Call the number above for answers to your questions, to explore treatment options, and to check insurance coverage.
Find Stimulant Addiction Treatment Centers
Finding facilities near you…
Finding facilities near you…
Finding facilities near you…
References
- Substance Abuse and Mental Health Services Administration. Key Substance Use and Mental Health Indicators in the United States: Results from the 2024 National Survey on Drug Use and Health. Center for Behavioral Health Statistics and Quality, SAMHSA; 2025. Accessed June 3, 2026. https://www.samhsa.gov/data/sites/default/files/reports/rpt56287/2024-nsduh-annual-national/
- Tanz LJ, Miller KD, Dinwiddie AT, et al. Drug Overdose Deaths Involving Stimulants — United States, January 2018–June 2024. MMWR Morb Mortal Wkly Rep. 2025;74(32). Accessed June 3, 2026. https://www.cdc.gov/mmwr/volumes/74/wr/mm7432a1.htm
- National Institute on Drug Abuse. Drug Overdose Deaths: Facts and Figures. NIDA; updated 2025. Accessed June 3, 2026. https://nida.nih.gov/research-topics/trends-statistics/overdose-death-rates
- American Society of Addiction Medicine; American Academy of Addiction Psychiatry. The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder. J Addict Med. 2024;18(1S). Accessed June 3, 2026. https://www.asam.org/quality-care/clinical-guidelines/stimulant-use-disorders
- Trivedi MH, Walker R, Ling W, et al. Bupropion and Naltrexone in Methamphetamine Use Disorder. N Engl J Med. 2021;384(2):140-153. Accessed June 3, 2026. https://www.nejm.org/doi/full/10.1056/NEJMoa2020214
- Coyle JR, Brent JT, Cohen HM, et al. Mirtazapine for the Treatment of Methamphetamine Use Disorder Among Cisgender Men and Transgender Women Who Have Sex With Men: A Placebo-Controlled Randomized Clinical Trial. JAMA Psychiatry. 2020;77(3):246-255. Accessed June 3, 2026. https://jamanetwork.com/journals/jamapsychiatry/fullarticle/2757018
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Publishing; 2013.
- Centers for Disease Control and Prevention, National Center for Health Statistics. Drug Overdose Deaths in the United States, 2023–2024. NCHS Data Brief No. 549. CDC; 2025. Accessed June 3, 2026. https://www.cdc.gov/nchs/products/databriefs/db549.htm




